Publication Information
ISSN: 2641-7049
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2018
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Unruptured intracranial aneurysm: case series report
Thiago Navarro*1, Oscar Raul Sarmiento2, Maria Sofia Gonzalez Casagu1, Ricardo Novoa Alvarez1, Jorge Andres Perez Lizcano1
1Fundacion Universitaria Navarra – UNINAVARRA, Department of Research in Neurosurgery and Neuroscience of the Research and Innovation Center CIINA – UNINAVARRA
2Endovascular Interventional Neurosurgeon of the Medilaser Clinic
Received Date: February 13, 2023; Accepted Date: March 17, 2024; Published Date: April 22, 2024
*Corresponding author: Thiago Andres Navarro Alvarez, MD Fundacion Universitaria Navarra – UNINAVARRA, Department of Research in Neurosurgery and Neuroscience of the Research and Innovation Center CIINA – UNINAVARRA
Citation: Navarro T, Sarmiento OR, Casagu MSG, Alvarez RN, Lizcano JAP (2024) Unruptured intracranial aneurysm: case series. Jr Neuro Psycho and Brain Res: JNPBR-191
DOI: 10.37722/JNPABR.2024203
Abstract
Background
Intracranial aneurysms are often diagnosed incidentally, so it is important to know as many details as possible regarding the factors related to their rupture and other features observable in diagnostic imaging studies. Our objective is to describe the characteristics of the aneurysm, its location and its relationship with the event of rupture or not.
Methods
On a total of 510 cases of patients diagnosed with aneurysm, data on age, sex and characteristics of the intracranial aneurysm such as location, diameter, neck length and whether it ruptured were recorded. For quantitative variables the mean difference test was performed, and possible correlations were explored, while for qualitative variables the chi-square test was applied.
Results
An average age of 57.6 years was determined for the 510 patients and a sex distribution of 73% for women. The average diameter of the aneurysmal sac was 8.3mm and the neck length was 2.5mm on average. Twenty-nine percent of the cases corresponded to patients with unruptured intracranial aneurysms. The most frequent location was the posterior communicating artery followed by the middle cerebral artery. Statistically significant differences were found in the mean age of patients with unruptured intracranial aneurysms (5.6 years older, p=0.001) and in the location, with the carotid artery being less likely to rupture.
Conclusion
Intracranial aneurysms have different risk factors for their formation and rupture. It is not yet possible to accurately predict the likelihood of hemorrhage given the contradictory findings in different studies and the multifactorial nature of aneurysm formation, growth and rupture.
Keywords: Unruptured aneurysm, intracranial, risk factors
Introduction
Unruptured intracranial aneurysm (UIA) are vascular abnormalities characterized by a weakened area in the wall of a blood vessel that results in a localized dilation or bulging. UIA has a prevalence of 2,3%-3,2% in general population (1), which is a fact that denotes the importance of this condition that has a high lethality potential. Understanding the significance of unruptured aneurysms involves considering both the potential risks associated with rupture and the challenges of managing them (2). Rupture can lead to subarachnoid hemorrhage (SAH) and can result in severe neurological complications, disability, or even death (3). Unruptured aneurysms are often discovered incidentally during diagnostic imaging for unrelated health issues or through screening programs. Many individuals with unruptured aneurysms may be asymptomatic, making the discovery incidental (4).
The risk of rupture is often associated with the size and location of the aneurysm (5). Larger aneurysms and those located in certain critical areas of the brain may pose a higher risk of rupture (6). Not all aneurysms warrant immediate intervention, and the approach may vary based on factors such as the patient’s age, overall health, size and location of the aneurysm, and the presence of other risk factors (7). Advances in medical imaging and monitoring technologies have enhanced the ability to detect and monitor unruptured aneurysms (8). This allows for more accurate risk assessments and better-informed decisions about the most appropriate management strategy for each individual patient (9).
For individuals with unruptured aneurysms, lifestyle modifications may be recommended to manage risk factors associated with aneurysm growth and rupture (10). These may include blood pressure control, smoking cessation, and other measures to promote cardiovascular health. Ongoing research contributes to a deeper understanding of the factors influencing the rupture of unruptured aneurysm. This research, coupled with clinical guidelines, helps healthcare professionals make informed decisions about the management of unruptured aneurysms and refine treatment strategies (11). The potential impact on the quality of life, including psychological well-being and the stress associated with living with the knowledge of an aneurysm, is an important consideration in decision-making and patient care (12).
We investigated the risk factors associated with the delayed detection of unruptured intracranial aneurysms (UIA) in a comprehensive and forward-looking study involving a large sample of the general population. Additionally, we incorporated patients who had experienced an aneurysmal subarachnoid hemorrhage (aSAH) to identify any potential variations in risk factors.
Methods
Because of the sensitive nature of the data collected for this study, requests to access the medical records from a health institution of SouthColombia Region. With permission from the Ethical, Bioethical and Research committee for medical and health care from the Health Institution. We reviewed the medical records that were registered with the CIE-10 code corresponding to intracranial aneurysm to collect clinical information related to medical history, the form of diagnosis and outcome of each case. The histories of patients with ruptured aneurysms were reviewed to compare the findings found in patients in whom the diagnosis of aneurysm was incidental. The review covered a 10-year period of patients treated in the city of Neiva and the city of Florencia, both in the south of the country. For qualitative variables, a descriptive analysis of frequencies, percentages and proportions was performed, while for quantitative variables, after verifying the normality of their distribution, mean difference and correlation analyses were performed, as appropriate.
Results
Unruptured Intracranial Aneurysm
A total of 510 cases of patients with aneurysms were found. The 27.2% were men and the remaining 72.8% were women. The mean age was 57.6 years with a standard deviation of 14.97 years (table 1). The mean age of women was 6 years older than that of men, which is statistically significant (Table 2). Similarly, the average age also shows a difference, being on average 6 years older for patients who did not have aneurysm rupture (Table 2). On the other hand, when analyzing the differences in location of the aneurysm (Figure 1) there is also a statistically significant difference in the case of the carotid artery, being more likely that in this artery the aneurysm does not rupture.
Table 1. Aneurysm Characteristics
| N | Min | Max | Mean | SD | |
| Age | 510 | 9.00 | 90.00 | 57.5745 | 14.97940 |
| Largest Diameter | 275 | 3.00 | 30.00 | 8.3127 mm | 4.55826 |
| Small Diameter | 275 | 2.00 | 25.00 | 6.4255 mm | 4.17117 |
| Neck Length | 275 | 1.00 | 8.00 | 2.4691 mm | 1.26792 |
| Sex | 510 | 139 Men | 27% | 371 Women | 73% |
| Hemorrhage | 510 | 361 Yes | 70,80% | 149 No | 29,20% |
Aneurysms were found in a total of 6 locations, the most frequent being the posterior communicating artery followed by the middle cerebral artery and the carotid artery (Figure 1). Unruptured aneurysms had no other statistically significant differences related to aneurysm neck characteristics, or aneurysm measurements.
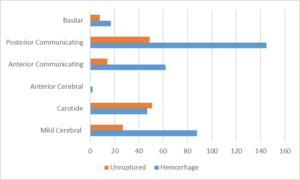
Figure 1. Unruptured aneurysm by location
Table 2. Risks Factors for hemorrhage
| Factor | Hemorrhage | Unruptured aneurysm | P-value |
| Age | 55,94 | 61,52 | <0,001 |
| Largest Diameter | 8,15 | 8,77 | 0,161 |
| Small Diameter | 6,37 | 6,59 | 0,349 |
| Neck Length | 2,4 | 2,68 | 0,06 |
| Calculated size | 68,6 | 71,52 | 0,418 |
| Location | Carotide | Others | 0,001 (pearson’s chi-square) |
| Sex | Men (76,98%) | Men (23,02%) | 0,06 (pearson’s chi-square) |
| Women (68,46%) | Women (31,54%) |
Discussion
Understanding the factors that contribute to the rupture of intracranial aneurysms is crucial. Investigative studies provide insights into the UIAs, helping healthcare professionals make informed decisions about monitoring, intervention, or surgical treatment based on factors such as aneurysm size, location, and patient characteristics (13). The exact reasons for the higher prevalence of intracranial aneurysms in women compared to men are not entirely understood. However, several factors have been suggested and studied, and it’s crucial to approach this explanation with the understanding that research in this field continues to evolve (14).
Hormonal factors, particularly those related to the menstrual cycle, pregnancy, and menopause, have been suggested as potential contributors. Changes in hormonal levels, such as fluctuations in estrogen, may influence the structural integrity of blood vessels, making them more susceptible to aneurysm formation (15). Estrogen, a hormone more predominant in women, is thought to have a protective effect on blood vessels by promoting vasodilation and maintaining vascular health. Fluctuations or declines in estrogen levels during different life stages, such as during menopause, may impact the vascular system and contribute to aneurysm formation. In general, the risk of intracranial aneurysm rupture leading to hemorrhage, particularly subarachnoid hemorrhage (SAH), is slightly higher in women than in men (16). However, it’s important to note that aneurysms can cause hemorrhage in both sexes, and the difference in risk is relatively modest.
While aneurysms can rupture at any age, the risk of rupture tends to be higher in older individuals. Older age is considered a risk factor for aneurysm rupture, and the incidence of subarachnoid hemorrhage (SAH) increases with advancing age (17). Aneurysms themselves can undergo changes over time. They may grow, become more fragile, and their walls may thin, increasing the risk of rupture. These changes are more likely to occur in older individuals with long-standing aneurysms.
The relationship between aneurysm size and rupture risk is a critical consideration in the field of neurosurgery. Neurosurgeons often assess aneurysm size as a key factor in determining the risk of rupture. While aneurysm size alone does not provide a complete picture of rupture risk, it is a significant predictor (18). In general, larger aneurysms tend to have a higher risk of rupture compared to smaller ones. There is often a positive correlation between aneurysm size and the likelihood of rupture. Small aneurysms, typically those less than 5 mm in diameter, are considered to have a lower risk of rupture.
Aneurysms in the intermediate size range, between 5 mm and 10 mm, may pose a moderate risk of rupture. Larger aneurysms, exceeding 10 mm in diameter, generally have a higher risk of rupture (19). Neurosurgeons may be more inclined to recommend intervention, such as surgical clipping or endovascular coiling, for large aneurysms to reduce the risk of rupture.
Besides size, the shape and morphology of the aneurysm are also important. Aneurysms with irregular shapes or those with wide necks may have an increased risk of rupture compared to more regular-shaped aneurysms of similar size (20). The location of the aneurysm within the cerebral vasculature is crucial. Some locations are associated with a higher risk of rupture, irrespective of size (21). For example, aneurysms at the anterior communicating artery and the posterior communicating artery are known to have an elevated risk, however in this case series there was no difference in rupture according to location, except for the case of defining a lower risk when the aneurysm is located in the carotid artery. Then, it is important to consider a combination of factors, including aneurysm size, location, morphology, patient age, and overall health, to determine the most appropriate course of action for each patient. Regular monitoring of aneurysms, especially those considered at lower risk, may be recommended in certain cases. The field of neurosurgery continues to evolve, and ongoing research contributes to a deeper understanding of the complexities surrounding aneurysm rupture risk.
References
- Cras TY, Bos D, Ikram MA, et al. Determinants of the presence and size of intracranial aneurysms in the general population: the Rotterdam study. Stroke 2020;51:2103–10.
- Hallikainen J, Lindgren A, Savolainen J, Selander T, Jula A, Närhi M, Koivisto T, Kellokoski J, Ylöstalo P, Suominen AL, Frösen J. Periodontitis and gingival bleeding associate with intracranial aneurysms and risk of aneurysmal subarachnoid hemorrhage. Neurosurg Rev. 2020 Apr;43(2):669-679. doi: 10.1007/s10143-019-01097-1. Epub 2019 Apr 10. PMID: 30972514; PMCID: PMC7186244.
- Korja M, Lehto H, Juvela S, Kaprio J (2016) Incidence of subarachnoid hemorrhage is decreasing together with decreasing smoking rates. Neurology. 87:1118–1123
- Hall S, Birks J, Anderson I, Bacon A, Brennan PM, Bennett D, Chavredakis E, Critchley G, Dow G, Downer J, Galea J, Grover P, Gurusinghe N, Helmy A, Kounin G, Mukerji N, Patel H, Patel J, Ross N, St George J, Teo M, Tolias CM, Tzerakis N, Uff C, van Beijum J, Veighey K, White E, Whitfield P, Bulters DO; ROAR Investigators. Risk of Aneurysm Rupture (ROAR) study: protocol for a long-term, longitudinal, UK multicentre study of unruptured intracranial aneurysms. BMJ Open. 2023 Mar 16;13(3):e070504. doi: 10.1136/bmjopen-2022-070504. PMID: 36927598; PMCID: PMC10030903.
- Liu Q, Li K, He H, Miao Z, Cui H, Wu J, Ding S, Wen Z, Chen J, Lu X, Li J, Zheng L, Wang S. The markers and risk stratification model of intracranial aneurysm instability in a large Chinese cohort. Sci Bull (Beijing). 2023 Jun 15;68(11):1162-1175. doi: 10.1016/j.scib.2023.05.001. Epub 2023 May 10. PMID: 37210332.
- Etminan, N., Rinkel, G. Unruptured intracranial aneurysms: development, rupture and preventive management. Nat Rev Neurol 12, 699–713 (2016). https://doi.org/10.1038/nrneurol.2016.150
- Algra AM, Lindgren A, Vergouwen MDI, et al. Procedural Clinical Complications, Case-Fatality Risks, and Risk Factors in Endovascular and Neurosurgical Treatment of Unruptured Intracranial Aneurysms: A Systematic Review and Meta-analysis. JAMA Neurol. 2019;76(3):282–293. doi:10.1001/jamaneurol.2018.4165
- van der Kamp LT, Rinkel GJE, Verbaan D, et al. Risk of Rupture After Intracranial Aneurysm Growth. JAMA Neurol. 2021;78(10):1228–1235. doi:10.1001/jamaneurol.2021.2915
- Liu Q, Li K, He H, Miao Z, Cui H, Wu J, Ding S, Wen Z, Chen J, Lu X, Li J, Zheng L, Wang S. The markers and risk stratification model of intracranial aneurysm instability in a large Chinese cohort. Sci Bull (Beijing). 2023 Jun 15;68(11):1162-1175. doi: 10.1016/j.scib.2023.05.001. Epub 2023 May 10. PMID: 37210332.
- Algra AM, Lindgren A, Vergouwen MDI, Greving JP, van der Schaaf IC, van Doormaal TPC, Rinkel GJE. Procedural Clinical Complications, Case-Fatality Risks, and Risk Factors in Endovascular and Neurosurgical Treatment of Unruptured Intracranial Aneurysms: A Systematic Review and Meta-analysis. JAMA Neurol. 2019 Mar 1;76(3):282-293. doi: 10.1001/jamaneurol.2018.4165. PMID: 30592482; PMCID: PMC6439725.
- Brown RD Jr, Broderick JP. Unruptured intracranial aneurysms: epidemiology, natural history, management options, and familial screening. Lancet Neurol. 2014;13(4):393-404. doi: 10.1016/S1474-4422(14)70015-8
- Etminan N, Rinkel GJ. Unruptured intracranial aneurysms: development, rupture and preventive management. Nat Rev Neurol. 2016;12(12):699-713. doi: 10.1038/nrneurol.2016.150
- Jin D, Song C, Leng X, Han P. A systematic review and meta-analysis of risk factors for unruptured intracranial aneurysm growth. Int J Surg. 2019 Sep;69:68-76. doi: 10.1016/j.ijsu.2019.07.023. Epub 2019 Jul 26. PMID: 31356963.
- Yu SCH, Cheng PW, Antonio GE, Chan SCC, Lau TWW, Ma HTG. Prevalence of unruptured intracranial aneurysms in the Hong Kong general population and comparison with individuals with symptoms or history of cerebrovascular disease. Hong Kong Med J. 2022 Feb;28(1):16-23. doi: 10.12809/hkmj209236. PMID: 35260496.
- Wan Z, Meng H, Xu N, Liu T, Chen Z, Sun Y, Wang H. Clinical characteristics associated with sentinel headache in patients with unruptured intracranial aneurysms. Interv Neuroradiol. 2021 Aug;27(4):497-502. doi: 10.1177/1591019920971977. Epub 2020 Nov 4. PMID: 33148104; PMCID: PMC8580530.
- Liu H, Guo W, Xiang S, Hu P, Sun F, Gao J, Zhang X, Wang P, Jing W, Zhang L, Yang X, Duan C, He M, Zhang H, Qu Y. The natural course of unruptured intracranial aneurysms in a Chinese cohort: protocol of a multi-center registration study in CIAP. J Transl Med. 2019 Oct 22;17(1):349. doi: 10.1186/s12967-019-2092-z. PMID: 31640726; PMCID: PMC6805494.
- Volovici V, Verploegh IS, van Doormaal PJ, van Es ACGM, Roozenbeek B, Lingsma HF, Lanzino G, Dammers R, Krisht AF. Growth of unruptured aneurysms: A meta-analysis of natural history and endovascular studies. J Clin Neurosci. 2021 Sep;91:343-349. doi: 10.1016/j.jocn.2021.07.034. Epub 2021 Jul 28. PMID: 34373050.
- Vitošević F, Milošević Medenica S, Kalousek V, Mandić-Rajčević S, Vitošević M, Lepić M, Rotim K, Rasulić L. CLINICAL CHARACTERISTICS AND MORPHOLOGICAL PARAMETERS ASSOCIATED WITH RUPTURE OF ANTERIOR COMMUNICATING ARTERY ANEURYSMS. Acta Clin Croat. 2022 Aug;61(2):284-294. doi: 10.20471/acc.2022.61.02.15. PMID: 36818935; PMCID: PMC9934047.
- Abdelkhalek H, Abdelhameed EA, Zakarea A, El Malky I. Predictors of flow diverter stent in large and giant unruptured intracranial aneurysms, single-center experience. Neurol Sci. 2022 Nov;43(11):6399-6405. doi: 10.1007/s10072-022-06336-w. Epub 2022 Aug 19. PMID: 35984605; PMCID: PMC9616764.
- Qi P, Feng X, Lu J, Wang J, Hu S, Wang D. Morphological Irregularity of Unruptured Intracranial Aneurysms is More Related with Aneurysm Size Rather Than Cerebrovascular Atherosclerosis: A Case-Control Study. Clin Interv Aging. 2021 Apr 20;16:665-674. doi: 10.2147/CIA.S301326. PMID: 33907388; PMCID: PMC8069126.
- Lombarski L, Kunert P, Tarka S, Piechna A, Kujawski S, Marchel A. Unruptured intracranial aneurysms: relation between morphology and wall strength. Neurol Neurochir Pol. 2022;56(5):410-416. doi: 10.5603/PJNNS.a2022.0053. Epub 2022 Jul 26. PMID: 35880660.