Publication Information
ISSN: 2641-6859
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2018
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Real-Time Evaluation of Cartilage Blood Flow by Ultrasound Can Predict the Timing of the Growth Spurt in Adolescent Athletes
Hiroaki Kijima1*, Shin Yamada2, Masashi Fujii1, Hidetomo Saito1, Naohisa Miyakoshi1, Yoichi Shimada1
1Department of Orthopedic Surgery, Akita University Graduate School of Medicine, 1-1-1 Hondo, Akita 010-8543, Japan
2Yamada Orthopedic Clinic, 6-1-21 Barajima, Akita 010-0065, Japan
Received Date: 12 April, 2019; Accepted Date: 23 April, 2019; Published Date: 02 May, 2019
*Corresponding author: Department of Orthopedic Surgery, Akita University Graduate School of Medicine, 1-1-1 Hondo, Akita 010-8543, Japan. Tel: +81188846148; Fax: +81188362617; Email: h-kijima@gd5.so-net.ne.jp
Citation: Kijima H, Yamada S, Fujii M, Saito H, Miyakoshi N, Shimada Y (2019) Real-Time Evaluation of Cartilage Blood Flow by Ultrasound Can Predict the Timing of the Growth Spurt in Adolescent Athletes. Adv Ortho and Sprts Med: AOASM-111.
Abstract
Most overuse injuries in adolescent athletes occur during the growth spurt. However, the timing of the growth spurt differs among individuals. Thus, the real-time evaluation of developmental stage and prediction of the timing of the growth spurt would be helpful to prevent overuse injuries. A total of 174 knees of 91 primary school students (77 male subjects, 14 female subjects) were examined in this study. The developmental stage and cartilage blood flow of the tibial tuberosity were examined using ultrasonography. It was found that cartilage blood flows were observed frequently at the point where ossification will develop, and they were correlated with the timing of the growth spurt. We believe that the prediction of the timing of the growth spurt by evaluation of the cartilage blood flow could help prevent overuse injuries in adolescent athletes.
Introduction
Sports athletes in primary school are in the developing stage, and they must pass through the growth spurt, unlike adult athletes. Their tendons are not inserted into hard bone, but into weak cartilage in the adolescent period. The flexibility of tendons and muscles is relatively decreased in the period of the growth spurt, because bones grow more than tendons and muscles. As a result, the excessive traction stress on the tendon or muscle attachment site, causing the damage or pain at their insertion point. This is one of the most common causes of sports injuries in the adolescent athletes. Therefore, there are injuries exclusive to the developing period.
We must be particularly careful about overuse injuries for athletes ranging in age from around 9 to 13 years, because the growth spurt tends to occur in this age group. Osgood-Schlatter disease (OSD) is a representative overuse injury in this period, whose cause is the excessive traction stress at the tibial tuberosity; the patella tendon attachment site. OSD is often downplayed because it rarely interferes with future daily living activities. However, it is important to prevent OSD because it decreases sports performance due to its pain and sometimes requires long-term discontinuation of sports activity.
The timing of peak height velocity differs by about 4 years among individuals [1]. Thus, the onset time of overuse injuries including OSD also differs among individuals. Therefore, it is very important for the prevention of overuse injuries in adolescent athletes to easily evaluate the developmental stages in real-time.
To evaluate the developmental stage, several methods have been used, for example evaluation of bone age on X-ray [2], by an increase in the curve of the speed of height increase [3], or by an information system called a neural network [4]. However, X-ray evaluation exposes athletes to radiation, and it is difficult to use X-ray examination devices in the sports setting. Moreover, prediction based on a height increase requires a long period of measuring height.
On the other hand, ultrasonography can non-invasively evaluate the developmental stages of the parts where overuse injuries can occur. In addition, ultrasonography can very easily be used in the sports setting. Furthermore, ultrasonography can evaluate cartilage blood flow, which is observed only until the period of growth, in real time using the Doppler method. Cartilage blood flow is expected to be related to the stage of development or the growth spurt period, because it is related to the timing of ossification [5].
The purpose of this study was to clarify the relationship between the stages of development or the cartilage blood flow of the tibial tuberosity and the growth spurt period, when overuse injuries occur most, as a new approach for the prevention of sports injury in the adolescent athlete.
Materials and Methods
A total of 174 knees (146 males, 28 females) of 91 adolescent athletes (77 males, 14 females) who participated in medical checkups for overuse injuries in one prefecture in Japan were examined in this study. The average age of these 174 knees was 11 years (8-12 years). The height and age of the subjects were checked first, and then the developmental stage and the cartilage blood flow of the tibial tuberosity of the subjects were evaluated using ultrasonography (Xario, Toshiba, Japan). Approval for this study was granted by the institutional review board of our university and subjects gave informed consent to participate.
Ehrenborg et al classified the degree of development of the tibial tuberosity in 4 stages [6]: the period before the appearance of the ossification nucleus (secondary ossification center) of the tibial tuberosity was classified as the cartilaginous stage (stage-C); the period after the appearance of the ossification nucleus (secondary ossification center) was classified as the apophyseal stage (stage-A); the period after the concrescence of the secondary ossification center and the epiphysis of the proximal tibia was classified as the epiphyseal stage (stage-E); and the period after the epiphyseal line was closed was classified as the bony stage (stage-B). Furthermore, in the present study, stage-A was divided into stage-A1, in which the secondary ossification center does not have an acoustic shadow, and stage-A2, in which the secondary ossification center has an acoustic shadow on the ultrasound images, and stage-E was divided into stage-E1, in which the secondary ossification center is combined with the epiphysis of the proximal tibia only partly, and stage-E2, in which the concrescence of the secondary ossification center and the epiphysis of the proximal tibia is completely finished. Therefore, the developmental stage of the tibial tuberosity was evaluated by classifying it into 6 periods in total (Figure 1, Figure 2).
 Figure 1: Evaluation of the tibial tuberosity with ultrasonography. The probe for ultrasonography is placed parallel to the patellar tendon, and the parts of the tibial tuberosity are observed with the longitudinal image.
Figure 1: Evaluation of the tibial tuberosity with ultrasonography. The probe for ultrasonography is placed parallel to the patellar tendon, and the parts of the tibial tuberosity are observed with the longitudinal image.
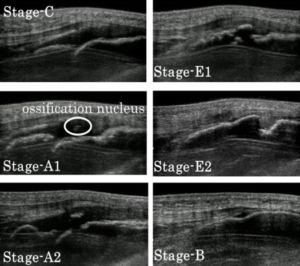
Figure 2: Ultrasonographic images of the tibial tuberosity. Stage-C is the period before appearance of the ossification nucleus, stage-A1 is the period when the secondary ossification center does not have an acoustic shadow, stage-A2 is the period when the secondary ossification center is accompanied by an acoustic shadow, stage-E1 is the period when the secondary ossification center is combined with the epiphysis of the proximal tibia only partly, stage-E2 is when the concrescence of the secondary ossification center and the epiphysis of the proximal tibia is completely finished, and the period after the epiphyseal line is closed is stage-B.
In addition, an abundant blood supply is observed in the cartilage during the period of the growth spurt by the ultrasonographic Doppler method [5]. Therefore, the cartilage blood flow of the tibial tuberosity was measured using the ultrasonographic Doppler method using the following 5 categories: F1 was defined as blood flow around the proximal tibial epiphysis; F2 was defined as blood flow that is prolonged to the epiphysis between the epiphysis and the secondary ossification center; F3 was defined as blood flow that is prolonged to the secondary ossification center between the epiphysis and the secondary ossification center; F4 was defined as blood flow that is prolonged to the secondary ossification center between the metaphysis and the secondary ossification center; and F5 was defined as blood flow around the metaphysis.
Results
Overall, 73 knees were stage-C, 42 were stage-A1, 13 were stage-A2, 23 were stage-E1, 19 were stage-E2, and 4 were stage-B. As the school year advanced, the developmental stages of the tibial tuberosity progressed (Figure 3). In addition, there was a strong positive correlation between the developmental stage of the tibial tuberosity and height; however, there was a 5 to 26-cm individual difference at the same stage of development (Figure 4). The average number of the cartilage blood flow in each stage showed a distribution with a peak with the highest number of the cartilage blood flow at stage-A2 (Figure 5). F1 was detected most often in stage-C, F2 was detected most often in stage-A1, F3 was detected most often in stage-A2, and F5 was detected in many cases in stage-A2 and stage-E1 (Figure 6).
 Figure 3: The developmental stage of every school year. As the school year advances, the developmental stage progresses.
Figure 3: The developmental stage of every school year. As the school year advances, the developmental stage progresses.
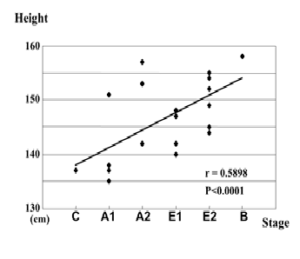
Figure 4: The relationship between height and developmental stage. Height and developmental stage have a strong positive correlation. However, there are individual differences in the same stages of development.

Figure 5: Cartilage blood flow in each developmental stage. The average number of cartilage blood flow shows a distribution with one peak at stage-A2

Figure 6: Cartilage blood flow according to the site in each developmental stage. F1 is detected most in stage-C, F2 is detected most in stage-A1, F3 is detected most in stage-A2, and F5 is detected in many cases in stage-A2 and stage-E1.
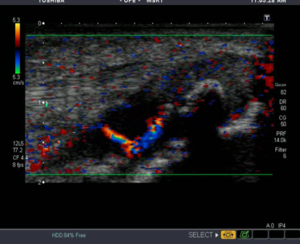
Figure 7: The ultrasound color Doppler image of the tibial tuberosity during the period when sports injuries occur easily. This is stage-A2, and there is abundant cartilage blood flow between the epiphysis and ossification nucleus.
Discussion
If we can evaluate the developmental stages of children in the growth period in real time in the sports setting, overuse injuries, which frequently occur in the period of growth, can be better prevented. In this study, it was found that the developmental stages and the cartilage blood flows of the tibial tuberosity could be evaluated with ultrasonography very easily during medical checkups for adolescent overuse injuries.
It has been reported that the main factor related to adolescent sports injuries, particularly OSD, is that the insertion of the tendons, for example the tibial tuberosity, is histologically weak in the apophyseal stage of the X-ray classification, namely stage-A2 in the present study [7,8]. Another factor is a decrease in flexibility due to the imbalance between the bones and the musculotendinous growth in the growth spurt period [9]. It has been thought that one year before and after the time of peak height velocity and 2-4 years after the secondary sexual characteristics appear are related to stage-A2 [1], because 80% of OSD develops one year before and after the timing of peak height velocity [1], and 70% of OSD develops 2-4 years after the appearance of secondary sexual characteristics, and the onset of OSD is affected by personal developmental stages.
The results of the present study confirmed that ultrasonography can easily and precisely evaluate developmental stages by scanning the tibial tuberosity. It was also suggested that stage-A2 represented the growth spurt period, because cartilage blood flow was the greatest, which is found to match the timing of ossification, in stage-A2. Furthermore, there is much cartilage blood flow around the proximal tibial epiphysis in stage-C, and the cartilage blood flow between the epiphysis and the secondary ossification center, where concrescence begins, increased in stage-A2, and it was the cartilage blood flow around the metaphysis that remained until stage-E. Therefore, it was found that cartilage blood flow increases where the ossification will progress. In other words, it was confirmed that cartilage blood flow was related to the timing of ossification. Thus, the period when abundant cartilage blood flow between the epiphysis and the secondary ossification center is observed is in stage-A2 (Fig.7), which was confirmed to be the growth spurt period and the danger period when overuse injuries occur the most. In this way, it was shown that the dangerous period for injury could be predicted by evaluation of the developmental stages and cartilage blood flow with ultrasonography. And at that dangerous period, active muscle and tendon stretch exercises should be able to prevent the overuse injury before the damage or pain occurs.
It will be necessary in the future to increase the number of cases and to investigate the length of each stage by evaluating the same individuals over time. In addition, this result will need to be applied clinically by examining cases in which injuries actually have occurred. Furthermore, if similar evaluations of other parts can be performed, individual training programs according to each part or according to each competition can be more precisely developed. The results of this study also lead to the prevention of all overuse injuries in adolescent athletes, as well as OSD, because individual training schedules can be developed more exactly according to each event or each body part when the real-time evaluation by ultrasound of cartilage blood flow is performed for many other parts.
References
- Suzuki E, Saito T, Morishita S (2006) The factors, treatments, and preventions of Osgood-Schlatter disease From the viewpoint of physical characteristics and the growth process. Rinsho Sports Igaku. 23: 1035-1043.
- Yashar A,Loder RT, Hensinger RN (1995) Determination of Skeletal Age in Children with Osgood-Schlatter Disease by Using Radiograph of the Knee. Journal of Pediatric Orthopaedics. 15: 298-301.
- Murata M (1988) Physiologic characteristics in the growth of the Japanese children- From Japanese-Chinese comparison. Rinsho Sports Igaku. 5: 979-984.
- Chinmoy P, Ichiro H, Naoki K, Shin M (1994) Dynamic system identification by neural network-A fast learning method based on error back propagation. Journal of Intelligent Materials Systems and Structures 5: 127-135.
- Yousefzadeh DK, Doerger K, Sullivan C (2008) The blood supply of early, late and nonossifiying cartilage: preliminary gray-scale and Doppler assessment and their implications. Pediatr Radiol. 38: 146-158.
- Ehrenborg G, Lagergren C (1961) Roentgenologic changes in the Osgood-Schlatter lesion. Acta Chir. Scand. 121: 315-327.
- Flowers MJ, Bhadreshwar DR (1995) Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J. Pediatr. Orthop. 15: 292-297.
- Ogden JA, Southwick, Wayne O (1976) Osgood-Schlatter’s disease and tibial tuberosity development. Clin. Orthop. 116: 180-189.
- Hawkins D,Metheny J (2001) Overuse injuries in youth sports: biomechanical considerations. Med. Sci. Sports Exerc. 33:1701-1707.