Publication Information
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2019
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
QOC Evaluation in CTC Harare
Kufakwanguzvarova Wilbert Pomerai1*, Mary Muchekeza2, Robert F Mudyiradima3, Notion Gombe1
1Faculty of Medicine, University of Zimbabwe, Zimbabwe
2Department Community Medicine, Midlands State University, Zimbabwe
3Masvingo Provincial Medical Directorate, Zimbabwe
Received Date: March 31, 2020; Accepted Date: April 05, 2020; Published Date: April 13, 2020
*Corresponding author: Kufakwanguzvarova Wilbert Pomerai, Faculty of Medicine, University of Zimbabwe, Zimbabwe. Tel: +2634303211; Email: pomeraiwilbert1@gmail.com
Citation: Pomerai KW, Muchekeza M, Mudyiradima RF, Gombe N (2020) QOC Evaluation in CTC Harare. Adv in Pub Health, Com and Trop Med: APCTM-108.
Introduction
This study was conducted in order to determine quality of care at Beatrice Infectious Hospital which was the largest and busiest Cholera Treatment Centre during the 2018 Harare Cholera outbreak. The aim was to assess compliance with the Zimbabwe Cholera Control Guidelines,(ZCCG) Ministry of Health and Child Care Quality Assurance policy as well as patient charter.
Methods: A descriptive study was conducted, Requirements in the ZCCG, the patient charter, and general literature where used to develop a checklist which was interviewer administered on patients who were randomly selected using the lottery method. Key informant interviews and observations were also used. Ethical issues such as beneficence, confidentiality and respect were maintained. No harm was inflicted on the patients. Patients had the right to stop the interview at any time. Epi info was used to analyze data.
Results: One hundred patients were recruited. Eighty percent of patients were managed as per protocol, monitoring of patients and documentation was weak, there was overcrowding in ward(less than 1m from each bed), there were separate wards for children, women and men, walls and floors were satisfactory, waste segregation was done well and color coding as well as labeling of bins was done as per guideline, foot baths were not standard, health worker morale was low due to late payment of salaries, majority(78%) reported care was fair, all patients reported that no clear times were communicated for medications and discharge
Discussion: Low staff morale may lead to negligence and negative outcomes, there is need to pay salaries in time. Cement floors and oil painted walls meant that cleaning and disinfection with water is easier and effective hence improved infection prevention and control (IPC). However overcrowding would compromise IPC and spread of diseases like Tuberculosis. Failure to communicate medication times and discharge times may lead to anxiety and dissatisfaction of patients and they may spread negative feedback to the community who may not come for treatment as a result. Weak documentation and monitoring of patients may lead to negative outcomes and miss learning opportunities through case audits. Compassion must be a leading force during outbreaks to promote quality, accountability and improved care
Definition of Cholera
Cholera is an acute diarrheal disease that can kill within hours if left untreated. [1, 3] According to the Zimbabwe cholera control guidelines, cholera is an acute bacterial enteric disease characterized by the sudden onset of profuse watery stool with or without vomiting; in untreated cases it may lead to rapid dehydration, acidosis, circulatory collapse, renal failure and hypoglycemia in children. Symptomatic cholera usually begins as profuse watery diarrhea without fever of abdominalcramps. The stool of cholera patients typically becomes a clear liquid flecked with white mucus, known as rice water stool. It is usuallyodorless or has a mild fishy smell. Vomiting which can be severe and painful leg cramps are common symptoms.
Researchers have estimated that each year there are 1.3 million to 4.0 million cases of cholera, and 21 000 to 143 000 deaths worldwide due to cholera [1].Most of those infected will have no or mild symptoms, and can be successfully treated with oral rehydration solution (ORS). Severe cases will need rapid treatment with intravenous fluids and antibiotics.Provision of safe water and sanitation is critical to control the transmission of cholera and other waterborne diseases.Urgent access to effective treatment in the form of approved antibiotics, ORS and intravenous fluids is key to save lives. Infection control and sanitation is also key to prevent further transmission or reinfection. On the 5th of September 2018 Harare city the capital city of Zimbabwe reported an index case that led to more than five thousand more cases being treated in various Cholera Treatment Centers (CTC).
Quality of Care in Health Defined
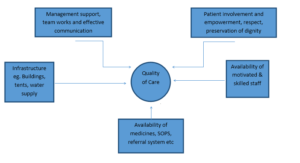
The World Health Organization defines quality of care as the extent to which health care services provided to individuals and patient populations improve desired health outcomes. In order to achieve this, health care must be safe, effective, timely, efficient, equitable and people-centered. [2] Safe as in delivering health care that minimizes risks and harm to service users and providers, including avoiding preventable injuries and reducing medical errors.Effective means providing services based on scientific knowledge and evidence-based guidelines. Times relates to reducing delays in providing and receiving health care.Efficient delivering health care in a manner that maximizes resource use and avoids waste.Equitablethat is delivering health care that does not differ in quality according to personal characteristics such as gender, race, ethnicity, geographical location or socioeconomic status. People centered meaning providing care that takes into account the preferences and aspirations of individual service users and the culture of their community. [2] Quality of care can be easily described using the below Quality of care conceptual frame work.
As stated below for quality of care to be experienced at CTC the following must be available in sufficient quantity and quality. Physical infrastructure is key this comes in the form of wards or tents for female’s male’s and children. Motivated skilled human resources for health has to be available in sufficient numbers so that they can take of the cholera patients timeously with dignity and respect as well as using the approved medicines by the authorities. Medicines and medical supplies must also be available in adequate quantities with reliable supply chain as well as approved by for example the medicines control authority of Zimbabwe (MCAZ). This is important for the safety of patients as well as effectiveness in treatment of patients so that admission time is reduced and resources of health system saved. SOPs must also be available and followed in this case ZCCG. Management commitment and support to quality, team work and effective communication need not be over emphasized for all the department must work together for the survival of the patient under support and monitoring from management. Patients who are the judges of quality must be involved as well in design and discharge of quality no matter the circumstance even in health emergencies and crisis. All this has to however occur in an robust health system. The lack or absence of these and any other elements key to quality increases the risk of lack of quality and negative outcomes like death in cholera and other treatment centres
 Measurement of Quality of Care in Health
Measurement of Quality of Care in Health
Quality has many definitions by so many authors , some say it is meeting or even exceeding patient needs and expectations, some say it is adhering to standards, others its zero defects , doing it right the first time and all the time others say quality is free. Many people defined in different ways, however, Institute of Medicine, National Academy of Science (US) defined as: The degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge [6]. In this study all the above definitions will be considered as true ti the meaning of quality. The researcher would also want to add another definition of his on which is; quality in health health care is when the health worker does all he or she can for the patient to the best of her ability and knowledge with the provision of the specified standards by law and regulatory bodies and also using the available resources with the expectation of saving the patient’s life or health.
It is very critical to always measure quality. Quality is a very difficult but critical parameter to measure especially and health emergencies and crisis as well as daily health care. This is so because patients do not know all about what must be done on them or to them for example there tests medications and so on they solely rely on the health workers’ professionalism and compassion. However quality is so subjective at times ad so difficult to measure.
In health care, quality improvement (QI) is the framework used to systematically improve the ways care is delivered to patients. Processes have characteristics that can be measured, analyzed, improved, and controlled. QI entails continuous efforts to achieve stable and predictable process results, that is, to reduce process variation and improve the outcomes of these processes both for patients and the health care organization and system. Achieving sustained QI requires commitment from the entire organization, particularly from top-level management. [4, 5] There is great need to measure and monitor quality in health crisis and emergencies such as cholera or Ebola.
There are different categories of quality in health care. These are namely, clinical quality which is relates to the interaction between health-care providers and patients and the ways in which inputs from the health system are transformed into health outcomes. Clinical quality has more to with health worker attitudes than availability of medicines and so on. [7, 8, 9, 10] There is process quality which how the patients judge quality of service despite not having medical expertise. This judgment can be based on friendliness of staff, politeness, information given on the ir condition, waiting time, cleanliness of the facility/ CTC which can be achieved through 5s philosophy, present ability of the health worker, availability of medications, whether the centre was organized or not. Perceived quality can lead to high utilization of cholera treatment centers or hospitals. [11,12] Due to lack of medical expertise as mentioned earlier patients may find it very hard to evaluate quality of care and makes most evaluations that are based on patient experiences inaccurate. [13, 14] Hence the need for triangulation. There is also process quality that looks at the activities or process that are carried out by health workers these could be procedures, examinations, giving medications, laboratory procedures procurement and so on. Them lastly the outcome quality which looks at the then what of the quality aspect. In this case it is the survival or death of the patients in the CTC.
There are so many ways of measuring quality, checklists may be used to assets availability of various inputs or whetherprocesses are done in CTC or other health crisis or emergencies. Check lists can be used to measure out comes. They are easy and fast as well cost effective questionnaires cane be used for the same purpose but can also be used to gather patients opinions in CTCs and other health and humanitarian crisis. Observations and inspections are also other methods to apply when trying to measure quality of care. Observation is good when trying to asses skills of health workers and also cleanliness and housekeeping in health camps or ETU or CTCs. Meetings with key informants and Focus Group Discussions (FGD) with patients can be used as especially to understand how the situation is on the CTC and also other detailed information and opinions of patients through FGDs. The collected data can then be analyzed and presented in graphs pie chats run chats etc. In this study only FGDs were not used out of all the above means. FGDs were not done because it was a humanitarian crisis the discharged patients needed to quickly go home and gathering not encouraged.
Recommended Management of a Cholera Patient According To Zimbabwe Cholera Control Guidelines (ZCCG)
The Zimbabwe cholera control guidelines (ZCCG) emphasizes on the need of rapid effective evidence based treatment for cholera by trained registered health care worker in order to have positive outcomes and reduce mortality as well as grouping cases in one centre in order to facilitate treatment using available staff and also prevent contamination. [3] The guidelines also states that the mainstay for cholera management is rehydration using ORS and IV fluids specifically Ringers lactate and Normal saline if ringers lactate is unavailable. Plain glucose fluids are highlighted as potentially dangerous. The ORS sachets are to be used as per the directions on the sachets. Cholera patients started on IV fluids must be given ORS as soon as they can start drinking even before the initial IV therapy has been completed. They should then be treated with ORS until the diarrhea stops. After rehydration patients should be allowed and encouraged to drink water.
The ZCCG advises health workers to asses severity of dehydration according to the diarrheas treatment chart (Dhaka method) Annex1. This were the health worker assess eyes, tongue, skin pinch, thirst, radial pulse if all is normal there is no dehydration and patient is sent home on 50 ORS mls per kg body weight over 6 hours plus ongoing loses. Second scenario is when there is some dehydration this is when the patient is irritable, less active, sunken eyes, thirst and drinks eagerly, skin pinch goes back slowly, reduced radial pulse there is some dehydration if at least any two of these signs are present and patients is given ORS 80 mls per kg body weight over 4-6 hours plus ongoing loses, patient should be kept under observation for six to twelve hours. Feeding must be continued with safe nutritious food. Dehydration status must be assed frequently (hourly). In case of vomiting frequently (>3 times in an hour) treat with IV fluid.
The third and most fatal condition is the severe dehydration where the patient condition is lethargic or comatose, unable to drink, skin pinch goes back slowly, uncountable or absent radial pulse, if some dehydration signs and any one of these are present classify as severe dehydration. The patient must be managed by immediate Ringer lactate (sodium potassium bicarbonate solution) 100ml/kg. For children under one year this must be 30mls/kg in the first hour, 70 mls/kg in next 5 hours. In adults the therapy is: 30 mls/kg in first half hour and 70mls/kg in the next 2.5 hours. The guidelines encourage patients to drink ORS as soon as they can and antibiotics after initial rehydration 4-6 hours. The ZCCG recommends the following antibiotics for management of severe dehydrated as follows;
First Line except In Pregnancy
For Adults: Ciprofloxacin, Tab PO 1g (500*2) single dose after correction of dehydration
For Children: Ciprofloxacin suspension PO 20mg/kg single dose after cessation of vomiting (if any)
Second Line
For Adults: Azithromycin Tab PO 1g (500*2) single dose after correction of severe dehydration.
For Children: Azithromycin suspension Po 20mg/kg single dose after cessation of vomiting (if any) There are also minimum requirements for a CTC in the ZCCG, as explained in annex 1 attached.
This study aimed at evaluating the compliance of patient care/Management, adhering to the ZCCG and also patient centeredness of services according to the ministry of Health Quality Assurance Policy and patient Charter in Harare city CTC during the 2018 cholera outbreak in Harare Zimbabwe
Methods
A survey was conducted on patients who were admitted in the three CTCs in Harare during the cholera outbreak. Sample size calculation was done using Dopson formula and the line list was use as sampling frame to systematically randomly select participants who were treated in the CTCs. An interviewer administered questionnaire was used to collected data. Interviews were done as exit interviews at discharge from the CTCs to prevent recall bias. Key informant interviews were done with health managers at CTC. Observation and inspections were done during working hours at the CTC to assess hygiene and also skills of patients as this is key on quality and infection prevention. The researcher also did records review of patients to assed documentation of management of cases as well as observation and inspections using a checklist. Data were analyzed using Epi info statistical package. Permission to carry out the study was sought and granted from relevant authorities. Patients were treated with respect, and privacy maintained. Frank feedback was given to the health managers and Ministry of Health.
Results
Assessment of CTC Compliance to the Cholera Control Guidelines
Clinical Management of Patients
Majority of the patients (80%) were managed as per protocol, however patient monitoring while on fluid replacement was weak and documentation was also weak among health workers. The average length of stay per patient was 4 days however documentation was also poor. It was noted that Azithromycin the drug of choice was out of stock at the beginning of the outbreak and this made length of stay longer since there was resistance to ciprofloxacin and doxycycline. Death audits were not conducted and clinical staff meetings erratic and documentation was poor. At the beginning of the outbreak patient nurse ratio was as high as 20 patients to 1 nurse.
Water and Sanitation
There was no adequate space ie 2m2 per person in the CTC, water supply both quantity and quality was adequate, free residual chlorine was satisfactory and tested three times a day, accessibility was satisfactory, mobile toilets wit doors and also flush system toilets for both males and female were satisfactory, adequate had washing facilities with disinfectants we satisfactory, both solid and liquid waste management was satisfactory, drainage was satisfactory since it was a functioning approved infectious hospital, communication with was weak and unsatisfactory, Clinical waste segregation and management was done and clear labels shown for easy identification. However rodents had access to the waste. Disinfection solution containers were marked and lebbled. Instructions on how to prepare solutions was displayed
Infrastructure
The entrance had foot baths that were not satisfactory as their with was not equal to 2 human steps, there was no schedule for changing dirty cotton blanket soaked in 2% chlorine solution, the depth of the foot baths was standard 5mm, entry was controlled and this is in line with guidelines, screening, triaging and observation areas were cleared separated and labeled this was consistent with the guidelines,
Wards
In the wards foot baths were not satisfactory as they lacked a width of two human steps, however water facilities, drainage, cholera beds and linen, buckets and water disposal system were satisfactory. However there was no documented standard schedule for monitoring waste disposal or stool removal. There were also separate wards and tents for female’s male’s and children. One of the female tents had no side flaps to prevent wind during the night. Storage of medicines sundries protective clothing, and disinfectants was satisfactory however stock cards were not updated in time. Medicines were clearlylabeled and easy to identify. There were no mosquito nets provided for patients
Kitchen
In the kitchen provisions were available and well managed and controlled by stock cards that were updated as per use, utensils were adequate though in the wards plastic plates and cups were used instead of ceramic and silver, cooking facilities were adequate, working space was satisfactory, hand washing facilities with soap available, food bins provided, solid and liquid waste management was satisfactory and also scullery. Ratusratus (rats) and baltnellagermanica (cockroaches) were present in the kitchen
Staff Office
Table and chairs were adequate and satisfactory for the staff, registers and stationery was available, there was no spot map displayed in CTC, line list was satisfactory and captured all patient information, List of staff and roaster with contact details was visibly displayed on the notice wall. No cleaning schedules were displayed.
Morgue
A proper morgue of the infectious hospital was used. Protective clothing, disinfectants, chloride of lime and body bags were satisfactory.
Waste Management
Colour coding was used, there was a selected waste storage zone fenced and locked, sewer system was satisfactory, some sharp waste material like catheters were seen on the ground and also bloody cotton wool, rodents had access to the waste area. No schedule for waste collection.
Documentation
Documentation was very weak. No cleaning, fly control, infection control procedure, operational procedure, roles definition was available. There was however a weak emergency preparedness plan (EPR) plan.Patients deaths were not audited.
Management Support, Motivated Skilled Staff Effective Communication and Team Work
Management support during the outbreak was fair as reported by the staff at the CTC and also by observation of the researcher. Resources were not adequate and management visibility was low. The staff was very demotivated as some had gone for three months without salary and cholera response allowances for the previous outbreak over ten years ago was not received. The employees could not hide their displeasure with management.
All employees had skills to manage cholera since they had done that before and also the training they received during the outbreak. Team work and communication was reported to be good and also based on the observations of the researcher the teams could try help one another and communicated well especially environmental health and nursing on infection prevention as well burial information and water quality testing in the suburbs.
Perception of Service by Patients in CTC
100 patients were interviewed, majority 60 (60%) were from Budiriro 1, followed by Glen view 30 (30%) and 9 (9%) were from othersuburbs. The median age was 26 years. Food was reported to be fair by majority of the patients 78 (78%), all patients reported that no clears times were mentioned for their medication by health workers 100 (100%), most patients 92 (92%)reported that doctors were coming late and not daily, some patients reported that they had to wait all day to be discharged later in the day, 81 (81%) reported that the CTC as clean , 76 (76%) reported that health workers were quick at triaging (5 to 10 minutes) and 88 (88%) reported that admission was slow. All the interviewed patients reported that the health workers were respectful and friendly. All the patients reported that Information on cholera was given adequately. However, the possible side effects of the medicines were not explained to the patients. Majority of patients reported that the services at the CTC was fair 83 (83%) and 17 (17%) reported that it was good.Turnaround time for laboratory results was also not given to patients,
Discussion
There was no documented target of patients to be managed as per guideline therefore the assumption was that all patients were supposed to be correctly managed as per guideline. The 20 % that was not managed as per guideline may have contributed tp deaths and longer patient stay. The non-adherence to guideline was associated to the shortage of the second line regiment during the early stages of the outbreak however it was later available. Weak monitoring of patients on fluid replacement which is the most critical intervention in management of a cholera vase was attributed to shortage of staff and high nurse patient ratio.The weak monitoring may lead to negative outcomes like death or longer hospital of stay and wastage of resources to manage the patient for more days. Meeting are crucial for information sharing updates, team building, joint planning, joint problem solving but however during those outbreak meetings were adhoc and also the guideline has not frequency of holding meetings during outbreaks. Clinical and death audits are critical learning meetings that were not being done during this outbreak and this may have led to the weak management of patients. There was adequate space between beds of 1m2 this is inline with international standards of hospitals and also infection control guidelines in Zimbabwe. The adequate space makes work easier for the health worker as they attend one patient to the other. Crowded beds make movement of health workers difficult as they try to squeeze their way between beds. There is some form of privacy as well since the beds will not be too close to each other.
Water quality and quantity was satisfactory this is key for a CTC because there must not be reinfection due to consumption of contaminated water. There is need for high standards of water safety and security in CTCs and this was met. The availability of safe portable water is a WHO requirement and also Public Health Act CAP15:07 1996 as amended. Patient recovery is made faster when there is safe water because main treatment of cholera is rehydration with safe water. Lack of safe water may lead to reinfection of patients and increased mortality.
The toilets availed to CTCs had doors and also lids to prevent flies from accessing the infected stool thereby reducing chances of cross infection and also spread of the disease. The availability of doors meant that patient privacy was observed and this in line with respect of patient dignity as outlined in the patients charter. Hand washing facilities had water and soap and this is in line with the infection control policy and guidelines. The availability of water and soap meant that patient and health worker safety was improved and risk of cross infection reduced. The unavailability of soap and adequate water would increase the risk of cross infection and increase harm on patient and health worker.There was no evidence of training of workers and also the application of the multimodal approach as stipulated in the infection control policy in Zimbabwe.
Waste management was done satisfactorily, there was segregation at source and that minimized infection control and also was compliant with infection control guidelines. Labeling of the various waste bins as well color coding meant less mistakes were done on the management of waste at the CTC. There were bin lids and bin liners available on the bins to prevent rodents from accessing the waste .if waste is accessed by rodents and flies it promotes cross infection and further the spread of cholera.
Rodents were seen on the CTC, this is a very dangerous situation as rodents can be vehicles of the spread of cholera because they can access stool containers and also bins and then patient or health worker food as well. During the time of the study we noted rodents and flies and the management was alerted of the situation. Rodents are also a nuisance under the public health Act.
Documentation was very weak. No cleaning, fly control, infection control procedure, operational procedure, roles definition was available. There was however a weak emergency preparedness plan (EPR) plan.The weak documentation leads to lost institutional memory on patient care or infection control and other key quality improvement activities. The absence of clear role definition may lead to poor performance as some activities may not be done or overlap and may lead to conflicts during outbreaks which is very detrimental to patients care as workers will be wasting time and energy on conflicts than patient care. The absence of documented procedures and standard operating procedure(SOP) may lead to variation and this may lead to negative patient outcomes.When employees have clear job descriptions they perform better and faster and there will be less conflict and patients outcomes are improved as well as the processes are done better and faster without friction.
The failure toaudit deaths in the CTC may have led to the relatively high number of deaths that happened in the CTCs. The culture of auditing deaths provide valuable learning opportunities that can lead to better management of patients and more positive patients outcomes. The practice of auditing deaths cultivates the culture of accountable patient care hence improved patient outcomes.
Management support during the outbreak was fair as reported by the staff at the CTC and also by observation of the researcher. Management commitment and support as well as visibility is very key for improved quality of care. The fact that management support and visibility was low may be associated with the state of affairs at the CTC that is resources were not adequate, the presence of strong leadership and their support during outbreaks can be a sustainable source of motivation for the employees and hence they perform their duties well. By its nature an outbreak needs all levels to be at the CTC and quick evidence based decision making is done promptly for the benefit of patients unlike when management is based in offices and at times not seen in the offices and decisions need to be made.
The employees could not hide their displeasure with management. Some of the staff was very demotivated as some had gone for three months without salary and cholera response allowances for the previous outbreak over ten years ago was not received. This made the staff do their tasks with less motivation and enthusiasm. It is known that employees who are paid well and on time perform better and have more commitment and they ensure that objectives of the Organisation are met for example in this case the objective was to provide quality health services to the cholera patients. All employees had skills to manage cholera since they had done that before and also the training they received during the outbreak. Trainings are very crucial for quality health services. The workers must have training that is commensurate with their duties and when this happens the employees will know what to do and do it with confidence and perception. There was one weakness as far as training was concerned and this was because there was no documentation of who was trained and also what they were trained and the training registers were not available.
Team work and communication was reported to be good and also based on the observations of the researcher the teams could try help one another and communicated well especially environmental health and nursing on infection prevention as well burial information and water quality testing in the suburbs.When there is team work performance and quality of care for patients is enhanced and likelihood for positive outcomes for patients is increase. The need for effective communication in outbreaks has to be strongly emphasized as this can lead to many mistakes and wastage on reworks. Unfortunately in health some errors may lead to loss of precious life. Food was reported to be fair by majority of the patients 78 (78%), This is very important because if the patients eat well because food is of good quality they recover early and the lack of good quality food can lead to poor feeding of patients and also waste due to left overs. All patients reported that no clears times were mentioned for their medication by health workers 100 (100%), the lack of communication with patients may be a sign of weak morale of staff. Lack of communication between health workers may lead to patients having anxiety of thinking when the medication will come etc and they may be stressed. It is important to have compassionate quality care program.
Most patients 92 (92%) reported that doctors were coming late and not daily, some patients reported that they had to wait all day to be discharged later in the day. In an outbreak it is very critical for proper quality of care to be delivered in time by qualified personnel. The fact that doctors were coming late for work during the outbreakmeant patient’s care was suffering and some negative outcomes may be experienced due to this. Late discharge of patients may lead to overcrowding of patients and infection prevention compromised.Longer stay in hospital may lead to more food consumption etc hence wastage.
Majority (81%) reported that the CTC as clean, Cleanliness of CTC may lead to satisfaction of patients, provide morale boost for health workers and also assist in infection prevention and control. In a CTC cleanliness is very critical and health workers are critical for the upkeep of the CTC. Most patients (76%) reported that health workers were quick at triaging (5 to 10 minutes) and 88 (88%) reported that admission was slow. Time is critical in managing cholera patients, delays may lead to death or complications of patients while they are in care of health workers in a CTC. Health workers were quick to triage but however took longer time to admit patients for proper management. There was no standard time set for each stage like triaging and between triaging and admission. Therefore the reported information is based on patient perception as per the SERVQUAL model.
All the interviewed patients reported that the health workers were respectful and friendly. Friendly and respectful health workers promote the much needed utilization of health services in this case CTC. If health workers are rude the discharged patients will then spread negative feedback to the community who will then shun the facility and cholera keeps on spreading and deaths happening. In this case quality becomes key in control of outbreaks. I have realized that if you are friendly to patients they tend to listen more to medical instructions hence adherence and recovery is faster this will then lead to shorter length of stay in hospital/CTC. All the patients reported that Information on cholera was given adequately. The provision of adequate cholera information is in line with the national patient charter and leads to easier control of cholera because information is power. The community and patients will be empowered if they have adequate correct information.
However, the possible side effects of the medicines were not explained to the patients. This could have been due to pressure and also focus on control of the outbreak rather than patient safety. The lack of side effects of medication may have led to the absence of adverse events register and poor documentation. The WHO is recommending patient safety in health services and it’s critical for the health workers to follow that in both normal and crisis health services provision.
Conclusion: Majority of patients reported that the services at the CTC was fair 83 (83%) and 17 (17%) reported that it was good.
Recommendation
Recommendation
Responsible person
Documentation of all medical procedures has to be strengthened during out breaks
Clinicians and management
Rodent and fly control measures to be adhered to all the time
Environmental Health
Medical/ officers to be available on CTC 24 hours during outbreaks
Harare city Management and Ministry of Health
Information of medicines sides effects to be given and register of rDocumentation of all medical procedures has to be strengthened during out breaks the side effects kept
Clinicians and Management
Adhere to the at least 1 square meter inter bed space to be maintained
Clinicians and environmental health
Schedule for cleaning of CTC and toilets to be developed and used
Management and environmental health
Take swabs of foot baths at stipulated intervals
Environmental health
Employee allowances to be communicated and paid on time as per communicated rate
Ministry of Health , City Health Management
References
- Ali M, Nelson AR, Lopez AL, Sack D (2015) Updated global burden of cholera in endemic countries. PLoSNegl Trop Dis 9(6): e0003832. doi:10.1371/journal.pntd.0003832
- https://www.who.int/maternal_child_adolescent/topics/quality-of-care/definition/en/
- Zimbabwe Cholera Control Guidelines 3rd Edition
- Mold JW, Gregory ME (2003) Best practices research. Fam Med 35: 131-134.
- Mold J, Peterson K (2005) Primary care practice-based research networks: working at the interface between research and quality improvement. Ann Fam Med 3: S12-S20.
- Source: IOM Definition of Quality (1990) http://iom.nationalacademies.org/Global/News%20Announcements/Crossing-the-Quality-Chasm-The IOM-Health-Care-Quality-Initiative.aspx
- WHO global strategy on people-centered and integrated health services. Geneva: World Health Organization; 2015. Available from: http://apps.who.int/iris/bitstream/10665/155002/1/WHO_HIS_SDS_2015.6_eng.pdf [cited 2016 Jun 10].
- Donabedian A (1980) Explorations in quality assessment and monitoring. The definition of quality and approaches to its assessment. Chicago: Health Administration Press; 1980.
- Institute of Medicine. Crossing the quality chasm: a new health system for the 21st century. Washington DC: National Academy Press; 2001.
- Donabedian A (1988) The quality of care. How can it be assessed?. JAMA 260: 1743-1748.
- Chang JT, Hays RD, Shekelle PG, MacLean CH, Solomon DH, et al. (2006) Patients’ global ratings of their health care are not associated with the technical quality of their care. Ann Intern Med 144: 665-672.
- Das J, Sohnesen TP. Patient satisfaction, doctor effort and interview location: evidence from Paraguay. Policy Research Working Paper No.WPS 4086. Washington DC: World Bank; 2006.
- Arrow KJ (1963) Uncertainty and the welfare economics of medical care. Am Econ Rev 53: 941-973.
- Arrow KJ (1986) Rationality of self and others in an economic system. J Bus 59: S385-399.