Publication Information
ISSN: 2641-7049
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2018
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Neurophysiology is what makes the Autistic Brain Different
David Rowland*
Independent Researcher registered with ORCID, Canada
Received Date: November 28, 2023; Accepted Date: December 11, 2023; Published Date: December 17, 2023;
*Corresponding author: David Rowland, Independent researcher registered with ORCID, Canada. Email: david222@hush.com
Citation: Rowland D (2023) Neurophysiology is what makes the Autistic Brain. Jr Neuro Psycho and Brain Res: JNPBR-181
DOI: 10.37722/JNPABR.2023201
Abstract
About 70% of those believed to be on the autism spectrum may not be autistic. This apparent epidemic of false diagnoses is being created by professionals who diagnose by ticking off symptoms on a checklist without questioning the causes of said symptoms, and without understanding the innate neurophysiology of the autistic brain. A dysfunctional cingulate gyrus (CG) hyperfocuses attention in the left frontal lobe (logical/analytical) with no ability to access the right frontal lobe (emotional/creative), which plays a central role in spontaneity, social behavior, and nonverbal abilities. Autistic people live in a specialized inner space that is entirely intellectual, free from emotional and social distractions. They have no innate biological way of emotionally connecting with other people. Autistic people process their emotions intellectually, a process that can take 24 hours, by which time it is too late to have felt anything. An inactive amygdala makes it impossible for autistic people to experience fear. Because they do not feel emotion, they have no emotional memories. All memories are of events that happened about which they felt no emotion at the time and feel no emotion when talking about it afterward.
Keywords: Autism, Asperger, Asd, Neurophysiology, Neuropsychology
Introduction
Definition: Autism is perpetual and unrelenting hyperfocus, the state of intense single-minded concentration fixated on one thing at a time to the exclusion of everything else, including one’s own emotions. The probable cause of hyperfocus is a dysfunctional cingulate gyrus (CG), that part of the brain which focuses attention. [1]
Description: Autism is an inherent neurophysiological difference in how the brain processes information. Autistic people live in a specialized inner space that is entirely intellectual, free from emotional and social distractions. They observe the world in detail without feeling any emotional attachment to what they see. [1]
Autism is a neurophysiological idiosyncrasy. The only thing different about an autistic brain is the specialized way in which it processes information. As such, autism does not fit the medical definition of disorder (i.e., pathological or diseased condition of mind or body). Michelangelo, Mozart, Paganini, Newton, Darwin, Jefferson, Edison, Tesla, and Einstein were autistic and obviously not suffering from any mental pathology. [2]
Historical Research
Autism, from the Greek word meaning self, was coined in 1911 by Swiss psychiatrist, Eugen Bleuler, who used it to describe withdrawal into one’s inner world.[3] Autistic children appear to be in a world of their own, isolated and alone with senses that can easily overload. These children talk endlessly about one subject, engage in repetitive behaviors (e.g., wringing hands, rocking body), continually repeat certain words or phrases (echolalia), and are resistant to change. [4]
In 1943, psychiatrist Leo Kanner studied the case histories of 11 highly intelligent children who shared a common set of symptoms consistent with autism: the need for solitude, the need for sameness, and to be alone in a world that never varied. [5] Kanner assumed that these children came into the world without innate biologically provided ways of emotionally connecting with other people. [6]
In 1944, medical professor Hans Asperger described “a particularly interesting and highly recognizable type of child” who has an autistic personality that is an “extreme variant of male intelligence.” Asperger described four boys who had severe difficulties of social integration that were compensated for by the kind of high level of thought or experience that can lead to exceptional achievements in later life. He chose the label autism for this condition as referring to an inherent fundamental disturbance of contact, the shutting off of relations between self and the outside world.[7] Asperger remarked that for those boys, social adaptation has to proceed via the intellect, and in fact they have to learn everything by the intellect. He considered the autistic syndrome to be a stable personality trait that is genetically transmitted in families. [8]
In 1962, psychiatrist Gerhard Bosch compared infantile autism to the Asperger autistic syndrome and considered them to be two variants of the same condition.[9] In the family of the author of this article, one young lad has nonverbal autism and his younger brother has Asperger’s, thus confirming that both variations have the same genetic origin.[2]
In 1979, psychiatrist Lorna Wing introduced the term Asperger syndrome to describe the autistic personality. Wing personally examined 34 cases fitting Asperger’s description of the autism syndrome and found that they had the following 11 traits in common: [10]
- Single-mindedness combined with social isolation;
- Pedantic speech, often consisting of lengthy discourses on favorite subjects;
- Poor comprehension of other people’s expressions and gestures;
- Tendency to misinterpret or ignore non-verbal signs;
- Impairment of two-way social interaction;
- Inability to understand rules of social behavior;
- Lack of the intuitive ability to adapt their approaches to fit in with the needs of others;
- Intensely attached to certain possessions;
- Excellent rote memories and intensely interested in one or two subjects;
- Absorb every available fact concerning their chosen field and talk about it at length, regardless if the listener is interested; and
- Thought processes are confined to a pedantic, literal, and logical chain of reasoning.
In 2020, David Rowland discovered that autism is caused by an inherent neurophysiological idiosyncrasy that creates a state of perpetual hyperfocus, which he defines as intense mental concentration fixated on one thought pattern at a time to the exclusion of everything else, including one’s own feelings.[11] Hyperfocus is the sole factor responsible for the autistic person’s withdrawal into an inner space that is entirely intellectual. Hyperfocus keeps a person’s awareness trapped in the analytical/logical left frontal lobe of the brain with no ability to access whatever may be happening in the right frontal lobe, the place where emotions and social connectivity are felt. Hyperfocus explains all 11 traits of Asperger syndrome as listed by Lorna Wing above.
The Spectrum Fallacy
Autism does not belong on any alleged spectrum. There is only one autism, and it is 100%. Either you are autistic, or you are not.
In 2013, the American Psychiatric Association merged the following four disorders under the umbrella of autism spectrum disorder (ASD): autism disorder, Asperger syndrome, childhood disintegrative disorder, and pervasive disorder not otherwise specified (PDD-NOS). This alleged spectrum is a basket catch-all for conditions of uncertain similarity.
The American Psychological Association defines autism spectrum disorder (ASD) as any one of a group of disorders typically occurring during the preschool years and characterized by varying but often marked difficulties in communication and social interaction.[12] DSM-5, the Diagnostic and Statistical Manual of Mental Disorders, describes autism as being characterized by (1) persistent deficits in social communication and social interaction; and (2) restricted, repetitive patterns of behavior, interests, or activities. These criteria are so vague as to be meaningless. If you do not know what causes certain symptoms, then you know nothing about any presumed disorder in question.
Epidemic of False Diagnoses
In 2018, the Centers for Disease Control (CDC) reported that 1 in 44 children were diagnosed with an autism spectrum disorder, for a prevalence rate of 2.27% of the population.[13] In 2012, a review of global prevalence of autism found 62 cases per 10,000 people, for a prevalence rate of 0.62%.[14] This apparent 266% increase in autism prevalence is in stark contrast to all other disorders in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), for which there have been no increase in prevalence over this same 6-year period.[15] These data suggest that 70% of those believed to be on the autism spectrum are not autistic.
A 10-year Swedish study in 2015 concluded that although the prevalence of the autism phenotype has remained stable, clinically diagnosed autism spectrum disorder has increased substantially.[16] Phenotyping is based on observing gene expressions in individuals and relating their conditions to hereditary factors. Nowadays professionals diagnose by ticking off symptoms on a checklist, without questioning the possible causes of said symptoms. This is a major step backward from clinical phenotyping.
A 2016 study reported that many children originally diagnosed with autism spectrum disorder were later found not to be autistic.[17] A comprehensive 2019 study in JAMA Psychiatry indicates that autism is being significantly over diagnosed.[18] Dr. Laurent Mottron, co-author of this study, has expressed these concerns: “The autism category has considerably overextended … most neurogenetic and child psychiatry disorders that have only a loose resemblance with autism can now be labelled autistic … you could not have ADHD and autism before 2013, now you can.”[19] Doctors now tend to label as autistic anyone who simply has ADHD and poor socialization. [20]
Neurophysiology of the Autistic Brain
The neurological structure of the autistic brain is the same as for any other brain. What is different about the autistic brain is how it functions with respect to its neurophysiology.
Table 1: Autistic Neurophysiology
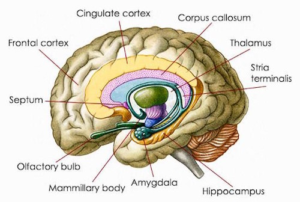
Cingulate Cortex/Gyrus
Dysfunctional
The cingulate gyrus (CG) is that part of the brain which focuses attention. In autism, the CG keeps the person’s attention trapped in the left frontal lobe, creating a perpetual state of hyperfocus.
Left Frontal Cortex/Lobe
Dysregulated
In the autistic left frontal lobe, alpha frequencies (8-12 Hz) predominate over beta (12.5-30 Hz), which is the exact opposite of the neurotypical brain. Higher alpha frequencies in the left brain appear to be compensating for the inability to access creativity and intuition from the right brain.
Right Frontal Cortex/Lobe
Inaccessible
There is normal brainwave activity in the right frontal lobe, with alpha frequencies predominating over beta. However, neural networks may be underdeveloped. The autistic person is completely unaware of anything that happens in his/her right frontal lobe, the place where emotions and social connectivity are experienced by neurotypical people.
Amygdala
Inactive
The amygdala plays a central role in the expressing of emotions, especially fear. A dysfunctional CG prevents the autistic person from feeling any emotion, with the result that the amygdala is non-functional. An autistic person never experiences fear.
In a neurotypical brain, the cingulate gyrus (CG) acts like an automatic transmission that seamlessly switches attention back and forth between frontal lobes, as needed. In autism, a dysfunctional CG keeps the person’s attention trapped in the left frontal lobe (logical/analytical) – with no ability to access the right frontal lobe (emotional/creative), which plays a central role in spontaneity, social behavior, and nonverbal abilities. Some neurotypical people are left-brain dominant whereas others are right brain dominant. Autistic people, however, are left brain exclusive. They speak factually, in a monotone voice, and with an expressionless face. [11]
The right frontal lobe, the place where emotions are experienced, is inaccessible to autistic people. The amygdala, the place where emotions are expressed, is inactive in the autistic brain.
These facts are consistent with Leo Kanner’s belief that autistic children come into the world without innate biologically provided ways of emotionally connecting with other people. [5]
In a neurotypical brain, the amygdala processes emotions associated with fear and stores emotional memories. When faced with a dangerous situation, the amygdala sounds an alarm that sets off a chain of events: hormones course through the body, pupils dilate, heartrate increases, and the body experiences a “fight or flight” reaction. In extreme situations, all nervous energy goes to the amygdala, which runs totally on instinct and emotion; and that part of the brain that uses logic shuts down completely. In the autistic brain, none of this happens because the amygdala is nonfunctional. In every dangerous situation, the autistic person is fully focused on the event itself and is incapable of feeling fear. Because autistic people do not feel emotion, they have no reaction and no emotional memories. All memories are of events that happened about which they felt no emotion at the time, and about which they feel no emotion when telling someone about it afterward.
Autistic people lack an emotional guidance system. They process their emotions intellectually, which process can take 24 hours, by which time it is too late to have felt anything. Physiological anxiety acts as a safety net to warn of any unprocessed emotion. Identifying and naming the emotion in question instantly relieves the anxiety.
Hyperfocus also causes various kinds of sensory overload. A sudden loud or high-pitched noise switches hyperfocus to the noise, which the autistic person then experiences with many times the intensity than does a neurotypical person. Seeing too many words on a page may cause cognitive impairment whereby the autistic person’s mind goes disturbingly blank. Too many products on shelves and overhearing unwanted conversations in stores may trigger anxiety. Lighting displays can trigger intense anxiety. For some, hyperfocus exaggerates the sense of touch, making close fitting clothing irritating and hugs unbearable.
Autistic Fearlessness
Autistic people have no involuntary fear response. Innate fearlessness makes autistic children oblivious to danger. In life-threatening situations, the autistic adult is fully focused on the event itself and incapable of feeling fear or even nervousness in that moment. She or he feels a mildly heightened sense of awareness while coldly calculating risks and mitigating factors that quickly form an immediate plan of action. The author of this article is autistic and in his entire life, including 17 years of experience in martial arts, has never once felt fear of any kind.[1] He has never had a fight-or-flight reaction and has no awareness of how that could feel.
Sometimes autistic people may intellectualize about fear, for example saying that after thinking about such-and-such decided it could be a scary thing. However, they are incapable of experiencing any actual fear. If you encounter someone who has never felt fear, this person is most probably locked into autistic hyperfocus. [1]
Litmus Test
Hyperfocus is the unique and defining causal state of autism that creates all of its observed characteristics. Hyperfocus prevents someone from dividing attention between two thought patterns or two stimuli at the same time. An autistic person talking to you is incapable of feeling any emotion in that moment. The surest way to find out if someone is autistic is to ask these five questions, to which you will receive the following responses.[1]
1.
How often do you cry?
“never” or “rarely”
2.
How often do you laugh?
“never” or “rarely”
3.
What are you afraid of?
“nothing” or an intellectual answer
4.
What are you feeling now?
“nothing” or an intellectual answer
5.
Do you ever get bored?
“never”
Anyone who answers all five questions as above is autistic. Anyone who answers four or fewer as above is not autistic.
50 Autistic Traits Have a Single Cause
Hyperfocus is the unique and defining characteristic of autism that is responsible for all 50 of its observed traits listed below. Hyperfocus is the perpetual and unrelenting state of intense single-minded concentration fixated on one thought pattern at a time, to the exclusion of everything else. All 50 of these traits are caused by the inability to run two mental programs simultaneously.[1]
Table 2: 50 Autistic Traits Caused by Hyperfocus · Trapped in thoughts, mind always busy · Tends to overthink everything · Passionately pursues interests, often to extremes · Amasses encyclopedic knowledge about areas of interest · Self-awareness but no social awareness · Interruptions trigger agitation, confusion, or anxiety · Cannot multitask · Sensory assaults can trigger physiological anxiety · Overwhelmed from hearing unwanted conversations · Overwhelmed by too much information · Sensory overload makes it impossible to think or focus · Difficulty listening to radio or talking with others while driving · Incapable of emotionally reacting to anything · Processes emotions intellectually · May have physiological responses instead of emotions · Anxiety bypasses the intellect to warn of unprocessed emotions · Incapable of experiencing fear · Can be angry without knowing so · Never (or rarely) cries or laughs · Cannot nurture self psychologically · Shrinks from emotional displays by others · Unable to defend against emotional attacks · Lacks innate ability to socialize · Unaware of feelings and needs of others · Oblivious to how perceived by others · Unaware of socially appropriate responses · Cannot pick up on subtleties, unable to take hints · Content of conversation important, context irrelevant · Speaks factually, without emotion · Takes everything literally · Easier to monologue than dialogue · Misinterprets sarcasm · Misses social cues and nonverbal communication · Participating in 3-way conversations may be overwhelming · May have difficulty following topic changes · May understand empathy but unable to feel it · Cannot be emotionally available to others · Others cannot provide an emotional safety net · Innate forthrightness tends to scare others · Never bored, always engaged in mental activity · Consistent to daily routines, agitated if routine is disturbed · Spontaneity not possible; activities must be pre-planned · Cannot lie spontaneously; can tell only premeditated lies
Mental Traits
· Intense single-mindedness
Sensory Overload
· Hypersensitive to loud noises and bright lights
Emotional Traits
· Biologically incapable of feeling emotion
Social Traits
· Considers self to be an outsider
In Conversation
· Interested only in information
In Relationships
· Understands love intellectually but cannot feel love
Temperament
· Drawn more strongly to certain things than to people
You cannot fix that which is not broken. The autistic brain works in a precise way that cannot be altered. [2] Therapy cannot change neurophysiology.
Applied behavioral analysis (ABA) therapy uses positive reinforcement to help autistic children learn behaviors that are deemed desirable. Reinforcement involves rewarding desired behaviors while discouraging undesirable behaviors.[21] There is a vocal community of adults with autism (many of whom had ABA as children) who say that ABA damages mental health and treats them as though they are a problem to be fixed. There is also a higher incidence of PTSD in autistic children who are exposed to ABA. [2]
ABA therapy ignores the child’s emotional well-being and quality of life. It assumes that children simply won’t do things and need to be incentivized to do them through rewards or lack of rewards. Therapists are unaware that autistic children cannot do what they are being asked to do, or that what they are being asked to do is painful. ABA therapy rewards autistic children to hide their pain and distress. [22].
There are increased symptoms of PTSD in children exposed to ABA therapy.[23] After repeated cycles in the classroom, autistic children begin to develop PTSD because the program focuses on behavior and compliance, and not what the children are communicating with their behavior.[24]
ABA is based on the cruel premise of trying to make autistic people “normal”. Its message is that autistic ways of doing things are wrong and need to be corrected, and that the autistic child is broken and must be molded to be more palatable to non-autistic people. This mistaken belief is destructive of the child’s identity and self-worth. [25]
ABA teaches autistic people that their needs are less important than pleasing others. This makes autistic children overly compliant, leaving them vulnerable to manipulation and abuse. These children need to be taught how to express and get their needs met, not to be taught that their needs are less valid than the needs of people around them.[2]
Differential Diagnosis
Differential diagnosis is distinguishing a specific condition from others that may have similar clinical features. The neurophysiological differences between autism and conditions for which it is mistaken are profound. [26]
Both attention deficit hyperactivity disorder (ADHD) and obsessive-compulsive disorder (OCD) share a common trait, fickle focus, which is defined as intervals of intense mental fixation interspersed with episodes of distraction or impulsiveness. Fickle focus can look like hyperfocus that comes and goes; however, true hyperfocus is perpetual and unrelenting. Autistic people never get any relief from hyperfocus.[2]
Because of the confusion between fickle focus and hyperfocus, many people with ADHD or OCD are misdiagnosed as being on the alleged autism spectrum. Also, some who are truly autistic are given false multiple diagnoses that include either ADHD or OCD or both.
Autism is entirely neurophysiological in origin. ADHD and OCD result from neurochemical imbalance. ADHD is caused by low dopamine.[27] OCD is caused by low serotonin.[28]
Table 3: Comparative Neuropsychology Processes emotions intellectually.
Autism
ADHD
OCD
Hyperfocus
Hyperfocus1
Fickle focus2
Fickle focus2
Cingulate Gyrus
Dysfunctional
Functional
Functional
Amygdala
Inactive
Active
Active
Left Frontal Lobe
High alpha activity.
High beta activity.
High beta activity.
Neurochemistry
n/a
Low dopamine
Low serotonin
Concentration
Intense
Intense
Intense
Distraction
Never distracted.
Sometimes distracted.
Self-distracts.
Multitasking
Unable to multitask.
May multitask.
Unable to multitask.
Emotional Aspects
Incapable of feeling emotion.
Can trigger intense emotions.
Compulsive behaviors may be attempts to alleviate emotional distress.
Social Aspects
Unable to understand and respond to emotional needs of others.
Poor social skills.
Social anxiety.
1Hyperfocus is perpetual attention fixated on one thought pattern at a time, to the exclusion of all else.
2Fickle focus is intervals of intense attention interspersed with episodes of distraction or impulsiveness.
Autism versus ADHD
Autism and ADHD are mutually exclusive. You can have one or the other, but not both. People with ADHD tend to be highly emotional. Autistic people are incapable of feeling emotion. Falsely believing autism and ADHD to be alleged co-morbidities is largely responsible for the epidemic of false diagnoses of autism.[19]
Intellectual Guidance System
Autistic people have no innate biologically provided way of experiencing emotions. What they have instead is an intellectual guidance system. They process their emotions intellectually, a process that can take 24 hours, by which time it is too late to have felt anything. Physiological anxiety warns of an unprocessed emotion. Identifying and naming the emotion in question instantly relieves the anxiety.[29]
Conclusions
What makes the autistic brain different is its unique neurophysiology (i.e., how it functions). The cingulate gyrus (CG) focuses attention exclusively in the left frontal lobe, creating perpetual and unrelenting hyperfocus, a state of intense single-minded concentration fixated on one thing at a time to the exclusion of everything else, including one’s own feelings.
Autistic people live in a specialized inner space that is entirely intellectual, free from emotional and social distractions. They observe the world in detail without feeling any emotional attachment to what they see. Autistic children come into the world without innate biologically provided ways of emotionally connecting with other people.
Autistic people lack an emotional guidance system. They process their emotions intellectually, a process that can take 24 hours, by which time it is too late to have felt anything. Physiological anxiety warns of an unprocessed emotion. Identifying and naming the emotion in question instantly relieves the anxiety.
Because the amygdala is inactive, autistic people are incapable of experiencing fear. Innate fearlessness makes autistic children oblivious to dangerous or life-threatening situations. In such situations, autistic adults may feel a mildly heightened sense of awareness while coldly calculating risks and mitigating factors.
References
- Rowland D. Redefining autism. Journal of Neurology, Psychiatry and Brain Research 2020; (02).
- Rowland D. Autism’s true nature. Journal of Neurology, Psychiatry and Brain Research 2021; (2).
- Blatt G. “Autism”, Encyclopedia Britannica.
- Montgomery S. Temple Grandin. New York, 2012: Houghton Mifflon Harcourt, p 22.
- Kanner L. “Autistic Disturbances of Affective Contact”. Nervous Child, 1943.
- Grandin T, Panek R. The Autistic Brain. New York: 2014, First Mariner Books, pp 5-7.
- Frith, U. Autism and Asperger Syndrome. Cambridge, 1991: Cambridge University Press, pp 37-92.
- Wing L. Asperger syndrome: a clinical account. Psychological Medicine 1981; (11):115-129.
- Bosch G. Infantile Autism (trans. D Jordan, I Jordan). New York, 1970: Springer-Vertag.
- Wing L. Asperger syndrome: a clinical account. Psychological Medicine 1981 ;( 11):115-129.
- Rowland D. The neurophysiological cause of autism. Journal of Neurology & Neurophysiology 2020; 11(5):001-004.
- “Autism spectrum disorder (ASD)”. APA Dictionary of Psychology.
- “Prevalence of autism spectrum disorder”. Surveillance Summaries, Centers for Disease Control and Prevention, Dec. 3, 2021. M, Di
- Elsabbagh M, Divan G, et al. Global prevalence of autism and other pervasive developmental disorders. Autism Research 2012; 5:160-179.
- Rowland D. Epidemic of False Diagnoses of Autism. Journal of Neurology, Psychiatry and Brain Research 2023 ; (01).
- Lundstrȍm S, Reichenberg A, et al. Autism phenotype versus registered diagnosis in Swedish children: prevalence trends over 10 years in general population samples. British Medical Journal 2015, Apr. 28.
- Blumberg SJ, Zablotsky B, et al. Diagnosis Lost: Differences between children who had and who currently have an autism spectrum diagnosis. Autism 2016; (7):783-95.
- Rodgaard E, Jensen K, et al. Temporal changes in effect sizes of studies comparing individuals with and without autism: a meta-analysis. JAMA Psychiatry 2019; 76(11):1124-1132.
- “Are We Overdiagnosing Autism”. com.
- Basu S, Parry P. The autism spectrum disorder ‘epidemic’: Need for biopsychosocial formulation. Australian and New Zealand Journal of Psychiatry 2013; 47(12):1116-8.
- “All about Applied Behavior Analysis (ABA) Therapy”. org.
- “Why ABA Therapy is Harmful to Autistic People”. com
- Kupferstein H. Evidence of increased PTSD symptoms in autists exposed to applied behavior analysis. Advances in Autism 2018 ;( 02).
- Grant A. Therapist Neurodiversity Collective: org
- “Rebelling Against a Culture that Values Assimilation Over Individuality”. com.
- Rowland D. Differential diagnosis of autism: a causal analysis. Journal of Neurology & Neurophysiology 2020; 11: 489.
- Wu J, Xiao H, et al. Role of dopamine receptors in ADHD: a systemic meta-analysis. Mol Neurobiol 2012; 45(3):605-20.
- Baumgarten HG, Grizdanovic Z. Role of serotonin in obsessive-compulsive disorder. Br J Psychiatry Suppl 1998 ; (35):13-20.
- Rowland D. Autism as an intellectual lens. Journal of Neurology, Psychiatry and Brain Research 2020 ;(01).
