Publication Information
ISSN 2691-8803
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2019
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Ludwig’s Angina with Pulmonary Koch’s And Severe Alcoholic Liver Disease with Ascites and Portal Hypertension: A Case Report
Tanveen Kaur Gill1*, Khattra M2, Chatha AK3, Sarin BC4
1Medical Graduate, SGRDUHS, Amritsar
2Junior Resident, Pulmonology Department, SGRDUHS, Amritsar
3Medical Student, SGRDUHS, Amritsar
4Head of Department, Pulmonology Department, SGRDUHS, Amritsar
Received Date: December 16, 2021; Accepted Date: December 24, 2021; Published Date: December 28, 2021;
*Corresponding author: Tanveen Kaur Gill, Intern, SGRDUHS, Amritsar, House No 1298, Sector- 68, SAS Nagar, Punjab, India, +91-9501459897. Email: tgill2060@gmail.com
Citation: Gill TK, Khattra M, Chatha AK, Sarin BC (2021) Ludwig’s angina with pulmonary Koch’s and severe alcoholic liver disease with ascites and portal hypertension: a case report. Adv Pub Health Com Trop Med: APCTM-141.
DOI: 10.37722/APHCTM.2021404
Abstract
Ludwig’s angina is a rare disease entity caused by diffuse cellulitis of neck space predominantly in the submandibular, sublingual and submental space. It can cause life-threatening complications as it spreads along the potential spaces of the neck to extend to the adjoining areas. The most feared complication of Ludwig’s angina is airway obstruction. Other complications include mediastinitis, carotid artery rupture, internal jugular vein thrombophlebitis, empyema, necrotizing fasciitis, osteomyelitis, and aspiration pneumonia. Early recognition and treatment of such patients can manage these patients well and prevent such life-threatening complications.
This case describes a 45-year-old man known case of Ludwig’s angina that evolved from a chronic dental infection. Upon the previous admission to another hospital, a diagnosis of Ludwig Angina was made and an Incision and drainage of the abscess were done. He later presented to the Emergency Department with complaints of fever, breathlessness on exertion and cough with expectoration for 4 days. Elective tracheostomy was done to prevent airway obstruction. While investigating the patient was diagnosed with multiple other comorbid conditions.
This case is exemplary for the successful management of this potentially lethal clinical condition. Our patient management is unique because three independent disease entities were managed simultaneously with excellent response. Early recognition and aggressive treatment helped to prevent the complications from Ludwig’s angina and prevent further progression.
Keywords: Antibiotics; Chronic Dental Infection; Ludwig’s Angina
Introduction
Ludwig’s angina is a rare disease entity caused by diffuse cellulitis of neck space predominantly in the submandibular, sublingual and submental space [1]. It predominantly affects Males in their 40s with low socioeconomic status [4, 5]. Most common aetiology is chronic dental infection. It can cause life-threatening complications as it spreads along the potential spaces of the neck to extend to the adjoining areas. The most feared complication of Ludwig’s angina is airway obstruction. Other complications include mediastinitis, carotid artery rupture, internal jugular vein thrombophlebitis, empyema, necrotizing fasciitis, osteomyelitis, and aspiration pneumonia [3].
Our patient, 45 years old male with Ludwig’s Angina, Pulmonary Koch’s, Alcoholic liver disease with ascites and Portal Hypertension was managed well and discharged in good condition. This case highlights the importance of how early intervention prevented the progression of life-threatening complications of airway obstruction from Ludwig’s Angina.
Case report
A 45-year-old male patient presented to the emergency department with complaints of fever, breathlessness on exertion and cough with expectoration for 4 days. The patient was a k/c/o Ludwig’s angina. History was suggestive of toothache (right lower second molar) for 5 months for which he had not sought medical advice. 5 days before admission he developed a swelling in the neck and high-grade fever for which he underwent incision and drainage and a diagnosis of Ludwig Angina was made. Post-op he started complaining of breathlessness, his saturation dropped to 85% and oxygen supplementation was started and he was referred to the Emergency Department. The patient had no history of Diabetes Mellitus/Tuberculosis/Bronchial Asthma. He was k/c/o hypertension which was not managed medically.
On presentation, his BP was 120/90, HR= 98 bpm with a RR of 24/min but he was afebrile. Systemic examination was done, and no significant finding was noted. His blood investigations were ordered, which were deranged with a TLC of 24000, serum creatinine of 2.18, serum bilirubin, direct bilirubin, SGOT, SGPT all raised. Viral markers were negative.
Radiological investigations were ordered, CXR revealed homogenous opacity in the left mid and lower zone and one in the right paratracheal region (Figure 1). CECT Chest was done, which revealed a loculated fluid collection in right carotid space tracking caudally along the right common carotid artery up till the aortic arch along with loculated fluid collection in the visceral space and a large pocket in the Danger space extending from the level of C1 caudally to the posterior mediastinum. Patchy areas of consolidation with air bronchograms involving the anterior and lingular segment of the left upper lobe were also seen (Figure 2). Radiological findings indicated the patient required a repeat incision and drainage along with elective tracheostomy to prevent airway obstruction.
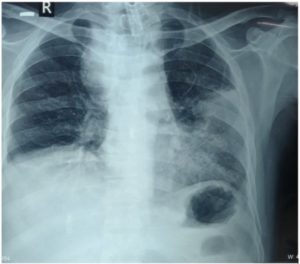
Figure 1: CXR revealed homogenous opacity in the left mid and lower zone and one in the right paratracheal region.
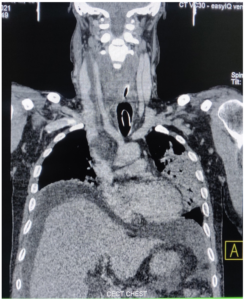
Figure 2: CECT Chest shows a loculated fluid collection in the right carotid space tracking caudally along with the Right Common Carotid Artery up till the aortic arch along with loculated fluid collection in the visceral space.
A sputum sample was collected and screened for mycobacterium tuberculosis, sputum for AFB was positive (+7 AFB) and sputum for Truenaat was also positive with rifampicin resistance not detected. The patient required anti-tubercular treatment. The patient was a chronic alcoholic and USG abdomen revealed hepatomegaly with liver showing slightly coarse echotexture and diffusely increased echogenicity with irregular margins at places along with moderate ascites and portal hypertension.
On admission, the patient was started on parenteral antibiotics including clindamycin, levofloxacin, linezolid, piperacillin-tazobactam and adequate hydration was maintained. Elective tracheostomy along with repeat incision and drainage of the abscess was planned. (Figure 3) He required diuretics, high protein diet to manage the symptoms of liver cirrhosis. Due to underlying deranged lfts, initially, only Isoniazid and Ethambutol were started and later once the lfts improved, DOTS without Pyrazinamide was started for tuberculosis.

Figure 3: Figure shows the tracheostomy tube and scar marks of Incision and Drainage.
The patient had a hospital stay of 29 days where he was managed for Ludwig’s angina, alcoholic liver disease along with ascites and portal hypertension and was started on ATT for pulmonary tuberculosis. On discharge, the patient’s blood investigations were all within normal limits, decannulation was done and the patient was advised to continue with ATT for a minimum of 6 months. The patient was advised for cessation of alcohol use and sought help for deaddiction. The follow up was scheduled after 5 days to review blood reports and revise the medications.
Discussion
Ludwig’s angina is a cellulitis of the submandibular, sublingual, and submental spaces, which tends to spread rapidly along the fascial planes. It is most commonly caused due to dental infection, although any other oropharyngeal infection has the potential to develop into Ludwig’s angina [3]. Such was the case with our patient who had a history of neglected toothache eventually resulting in Ludwig’s angina. He was a known case of hypertensive which aggravated the infection further as it has been found in previous researches that systemic diseases like diabetes mellitus and hypertension can increase their severity [7].
Our patient’s situation was unique in that he was inflicted with 3 independent diseases which had all been diagnosed within his 29-day hospital stay. Ludwig’s angina was managed with intravenous antibiotics and incision and drainage. He initially presented in a state of sepsis but responded to the antibiotics and draining the collection aided significantly as has been recommended to improve the prognosis [9]. Airway was maintained with elective tracheostomy as findings from retrospective literature have advocated the use of an elective awake tracheostomy as a safer alternative than endotracheal intubation [8].
The patient was also diagnosed with Pulmonary Koch’s whose spread is via droplet mechanism. History suggestive of chronic alcoholism predisposed the patient to develop liver cirrhosis which decompensated leading to ascites along with hypoalbuminemia and portal hypertension. He required diuretics, high protein diet to manage the same. Upon improvement in the previously deranged LFT patient could be started on ATT.
All three diseases posed a challenge as they limited the drug spectrum which could be used in the management of this patient. During the ICU stay, monitoring of blood labs along with timely intervention helped manage this patient and was discharged in good condition with all investigations within normal limits.
References
- Candamourty R, Venkatachalam S, Babu M, Kumar G (2012) Ludwig’s angina–an emergency: a case report with literature review. J Nat Sci Biol Med. 3:206-208.
- An J, Madeo J, Singhal M (2021) Ludwig Angina. In: statpearls [Internet]. Treasure Island (FL): statpearls Publishing.
- Kovalev V (2020) A Severe Case of Ludwig’s Angina with a Complicated Clinical Course. Cureus. 12:7695.
- Almutairi DM, Alqahtani RM, Alshareef N, Alghamdi YS, Al-Hakami HA (2020) Deep neck space infections: a retrospective study of 183 cases at a tertiary hospital. 12:6841.
- Karkos PD, Leong SC, Beer H, Apostolidou MT, Panarese A (2007) Challenging airways in deep neck space infections. Am J Otolaryngol. 28:415-418.
- Lin QL, Du HL, Xiong HY, Li B, Liu J et al. (2020) Characteristics and outcomes of Ludwig’s angina in patients admitted to the intensive care unit: A 6-year retrospective study of 29 patients. Journal of Dental Sciences. 15:445-50.
- Parhiscar A, Har-El G (2001) Deep neck abscess: a retrospective review of 210 cases. Annals of Otology, Rhinology & Laryngology. 110:1051-4.
- Balance E, Birch S (2018) Comparison of outcomes in conservative versus surgical treatments for Ludwig’s angina.