Publication Information
ISSN: 2641-693X
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2018
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Intravascular Leiomyomatosis of the Lower Vein Cava Extended to the Right Atrium
Rios William1, Rios Giovanny2*, Correa Juan2
1Cirujano Cardiovascular Pontificia Universidad Javeriana, Hospital de San José, Colombia
2Cirujano Cardiovascular Hospital Universitario de San Ignacio, Jefe de servicio de Cirugía
Cardiovascular Hospital Universitario de San Ignacio, Colobia
Received Date: November 04, 2019; Accepted Date: November 08, 2019; Published Date: November 19, 2019
*Corresponding author: Rios Giovanny, Cirujano Cardiovascular Hospital San Ignacio- Hospital San José, Profesor Asistente Pontificia Universidad Javeriana, Colombia. Email: edgar.rios@javeriana.edu.co
Citation: William R, Giovanny R, Juan C (2019) avascular Leiomyomatosis of the Lower Vein Cava Extended to the Right Atrium. Int Jr Cardiac Sci and Res: IJCSAR-114.
Summary
Intravenous leiomyomatosis is a rare condition that presents extension uterine gonadal veins entering the inferior vena cava to the right heart chambers, patients are usually asymptomatic and cause significant symptoms for pulmonary embolism or valve lesions by intracardiac obstruction. With high mortality in these cases.
Case: 38-year-old who presents with abnormal uterine bleeding, within their preoperative studies; transthoracic echocardiogram evidenced by mass in the right atrium, mobile that is inserted into the right ventricle; possible origin of atrial wall. It takes abdominal CT angiography which reports mass extending from the left iliac vein and travels through the inferior vena cava to the right atrium. It is carried in a first cardiac surgery with no evidence sternotomy thereof in any of the heart chambers. It is carried back a second surgical time when hysterectomy is performed, and exploration of the left common iliac vein is performed; showing soft dough, white, mobile color. Simultaneously transesophageal echocardiogram where the mass is reaching the right atrium and retracts into the inferior vena cava is performed. It is possible to remove intravascular mass of approximately 18 cm in length. Echocardiography is performed with no evidence of residual mass. Pathology report which is positive for intravascular leiomyomatosis. Adequate postoperative course.
Conclusion: This is an important case because of its rarity and operation set of various specialties and complexity of the surgical management with adequate postoperative course.
Keywords: Intravascular Leiomyomatosis; Right Atrium
Introduction
Intravascular leiomyomatosis is a rare condition that consists of proliferation of the smooth muscle which extends from the gonadal veins and can create large masses [1,2] with invasion from the mimes with a path from them; passing through the inferior cava vein and with compromise of the cardiac cavities [3], this can occur in 45% of the reported cases, it may be associated with trombosis of the adjacent tissue [4, 6].
Additionally, the symptomatology presented by the patients is not clear, this type of mass is usually evidenced incidentally [4, 5]. At the moment in which the patients present symptoms they are related to the complications which are severe given by massive pulmonary embolisms; Tricuspid valve obstruction and dysfunction [5, 7].
The multidisciplinary diagnosis as well as the surgical management which and in the cases reported is made in two stages; having as a first intervention the resection or cardiac exmination and after this the joint performance of hysterectomy and definitive intravascular resection by abdominal route as the one performed in our case.
We present the following case reporte of intravascular leiomyomatosis.
Clinical Case
This is a 38-year-old female patient who consults due to a clinical picture of abnormal uterine hemorrhage. She is evaluated by the gynecology department who programs for hysterectomy; within pre-surgical studies and taking into account the multiple comorbidities of the patient. Echocardiogram after thoracic is performed, showing mass of regular edges in the right atrium of approximately 8 cm x 6 cm, mobile; (Figure 2), of possible neoplastic origin adhered to the atrial wall. After this, abdominal angiotac is taken, where there is evidence of mass that occupies intravascular space from the right common iliac vein extending through the inferior vena cava and reaching the right atrium (Figure 1).
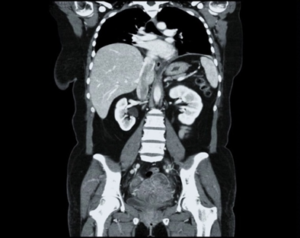
Figure 1: Abdominal CT scan showing mass in the Inferior cava vein to the right atrium.

Figure 2: Echocardiogram showing right atrial mass.
In the first stage, cardiac surgery is performed by performing sternotomy and exploration of the right atrium without evidence of such mass, or signs of intracardiac thrombosis. It is evaluated with a new echocardiogram finding persistence of the atrial mass without another significant sign. It is carried out to a second surgical time by abdominal route in a multidisciplinary way by oncological gynecology for hysterectomy and subsequent exploration in a controlled way of the left common iliac vein; simultaneously, it is evaluated with transesophageal echocardiography to monitor possible emboli and documentation of intravascular mass travel. Complete extraction of the dough with a length of approximately 18 cm in a cylindrical shape is achieved. (Figure 3). The complete extraction and non-occupation of the cardiac cavities are evaluated with echocardiography. Another fragment is extracted from one of the gonadal veins of the same characteristics.
Patient with adequate postoperative evolution and is in controls.
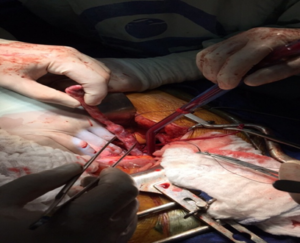
Figure 3: Intravascular Mass Extracted.
Final pathology report which shows and confirms intravascular leiomyomatosis (Figure 4).
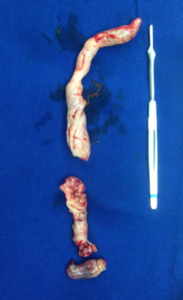
Figure 4: Surgical piece.
Discussion
Intravascular leiomyomatosis is an entity derived from uterine myomatosis which grows with invasion into the vessels, it is a proliferation of smooth muscle cells. This tissue proliferation is benign. The first cases were described in 1975 by Parmley [1, 3, 6]. Because it is a rare entity, it is not known what its etiology is. It should be taken into account that the complications given by massive pulmonary embolization and cardiac lesions caused by mass mobilization; they are severe and cause the death of patients [1, 5, 7].
The clinic of the patients is nonspecific given by dyspnea, syncopes, arrhythmias, dysmenorrhea in most cases and as ours are found incidentally [4, 5, 8].
The treatment is surgical, the complete extraction of the intravascular mass must be done due to the high embolic irrigation [3]. In our case, a first surgical time was performed as described with intracardiac examination to extract it; entering through the right atrium. A second time by abdominal route to perform hysterectomy and controlled venous exploration, complete extraction of the mass and verification by cardiology with echocardiography and to be certain of complete resection and non-pulmonary embolization of the same [2, 3].
The management of this pathology should be done interdisciplinarity given the complexity. In our case, an intervention was carried out by the services of oncological gynecology, cardiology and cardiovascular surgery which led to the intravascular and cardiac extraction of the mass [3, 5].
Conclusion
It is a complex pathology with a low incidence, multidisciplinary management, with a nonspecific clinic and mostly incidental diagnosis. In this way it shows an important challenge for the diagnosis and definitive management. High mortality due to pulmonary and cardiac complications must be taken into account.
References
- Vega AF, Ortiz F, Morales A (2013) Leiomiomatosis intravenosa. Reporte de caso. Rev. Medica. Sanitas 16: 134- 141.
- Mertens R, Valdés F, Muñoz C, irarrázaval M, Brañes J, Riquelme C, et al. (2012) Leiomiomatosis intravenosa de origen pelviano con extensión intracardiaca. Reporte de dos casos. Rev Med Chil 140: 906.
- Domingo Yagu ̈e-Romeo, Celia Bernal-Lafuente, Elena Angulo- Hervias (2010) Leiomiomatosis intravascular, Servicio de Radiologia, Hospital Universitario Miguel Servet, Zaragoza.
- Labbe J, Pumarino A, Ibarra J, Merello l (2014) Tumor intracardiaco presentación de leiomiomatosis intravascular. Unidad de ciruhia cardiovascular. Rev. Chilena de cardiologia 33: 61-66.
- Norris HJ, Parmley T (1975) Mesenchymal tumors of the uterus: intravenous leiomyomatosis. A clinical and pathologic study of 14 cases. Cancer 36: 2164-2174.
- Le Bouedec G, Bailly C, Penault-Llorca F, Fonck Y, Dauplat J (1999) Intravascular leiomyomatosis of uterine origin. A case of pseudo-metastatic cavo-cardial thrombus. Presse 28: 1463-1465.
- Gaudino M, Spatuzza P, Zinder F, Luciani N, Cina G, Posthay G (2002) Surgical management of a uterine leiomyoma extending through the inferior cava into the right Heart. Heart & Vessel 17: 80-82.
- Ruiz-Nodar JM, Aguilar Torres R, Nieto S, Iturralde E, Romero C, Jiménez J, et al. (1997) Leiomiomatosis intravenosa con extensión a cavidades derechas. Rev Esp Cardiol 50: 451-454.