Publication Information
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2019
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Fostering Clinical Reasoning through Critical Reflection in Doctor of Physical Therapy Education Using International Service-Learning in Honduras
Todd Watson*, Jessica Graning, Tim Eckard
Department of Physical Therapy, Western Carolina University, Cullowhee, NC, USA
Received Date: April 15, 2020; Accepted Date: April 21, 2020; Published Date: May 01, 2020
*Corresponding author: Todd Watson, Department of Physical Therapy, 228 Health and Human Sciences Building, Western Carolina University, Cullowhee, NC 28715, USA. Tel: +18282272126; E-mail: twatson@wcu.edu
Citation: Watson T, Graning J, Eckard T (2020) Fostering Clinical Reasoning through Critical Reflection in Doctor of Physical Therapy Education Using International Service-Learning in Honduras. Adv in Pub Health, Com and Trop Med: APCTM-110.
Abstract
Community engaged international service-learning (ISL) is becoming more popular in physical therapy education as it serves as a powerful conduit for students to gain relevant practical and clinical experiences and cross-cultural dialogue, enhance their local and global citizenship, and promote self-awareness through intentional critical reflection. Previous studies have described the development of reflection in students across health care disciplines, yet none have specifically examined the level of critical reflection in doctor of physical therapy (DPT) students in response to an ISL course. This exploratory study found student reflection papers regarding their ISL travel course experience to be written at the highest levels (reflective and critically reflective) using the Kember scale. No differences in levels of reflection were identified for age, gender or years in the DPT program. Recommendations are made for ISL travel courses that seek to develop clinical reasoning for their professional healthcare students as a student learning outcome for the course.
Keywords: Critical Reflection; Health Promotion; Honduras; International Service-Learning; Physical Therapy
Introduction
Physical therapist education endeavors to train competent practitioners for a vast array of health care settings, including practicing in a global health care environment [1]. Community engaged international service-learning (ISL) has become increasingly popular over the past decade in physical therapist education as faculty have begun to see the power of the results their students take from the experiences, so much so the American Physical Therapy Association has published an “International Service Manual for Students: A guide for students considering international service trips” [2]. This manual helps the student physical therapist or physical therapist assistant select and prepare for an ethical, sustainable study abroad service-learning course or experience. Bringle and Hatcher [3] defined ISL as a structured academic experience in another country having the following three elements in which students 1) participate in an organized service activity that addresses identified community needs; 2) learn from direct interaction, gain from practical experiences and cross-cultural dialogue with others; and 3) critically reflect on the experiences in such a way to gain further understanding of course content, a deep understanding of global and intercultural issues, a broader appreciation of the host country and the discipline, and an enhanced sense of their own responsibilities as citizens locally and globally. Community engaged learning is described as not merely service in a community that is for learning; but is collaborative, i.e. it is service-learning as described above with the community so that students, faculty and community members share decisions in planning and implementation for mutual benefit [4-8].
International experiences (service-learning and others) are increasingly popular throughout higher education, with study abroad participation doubling in the years 1999-2014 [9]. It is well documented that study abroad positively effects student’s careers, with specific enhancement of transferable skills [10]. Recent studies demonstrate that an ISL program promotes the students’ self-awareness through examination of their own beliefs and values through intentional reflection, such as considering the harsh economic poverty of the people with whom they worked compared with their own resources and lifestyles [11, 12]. Over the last decade many physical therapy educational programs have added international experiences and opportunities to their curricula including ISL, international clinical education experiences, and global health issues courses for their students [13-16].
Reflection is the process of hindsight, looking back on an experience and assessing its correspondence with existing meaning, thereby creating new meaning [17]. Evidence suggests that reflection positively enhances learning by reducing error rates in academic work and increased levels of personal success and happiness [18]. Additionally, students who reflect on their learning have been found to be more active in the learning process, have improved self-awareness and self-regulation, and demonstrate greater complexity in their thinking [19, 20]. In view of the predominantly experiential character of ISL education, student’s critical reflection of hands-on, practical experiences is an essential element for the processing and development of learning during and after their time in-country. ISL education is regarded as the means by which the educational experience is primed for transformative learning, pedagogically staging opportunity where, “reflection and critical reflection become imperative to the learning process” [21]. Critical reflection and its guided process through written form, go well beyond the “what” of what was learned and moves to the big picture perspectives of “so what?” (Why was that educational experience important to me?), and “now what?” (What behaviour changes or actions will I take from the experience?). It is the critical reflection process that can lead to a deeper understanding of how much more one has to learn about oneself, others, and the global society [22].
Purpose
The purpose of this exploratory study was to investigate the robustness of critical reflection occurring by doctor of physical therapy students in response to an ISL which took place in Honduras with an established community engaged program which occurred during a two-year time span. The value of reflection as a teaching strategy that promotes critical thinking, clinical reasoning, and improved clinical practice performance is well supported in the literature, [12, 23, 24] and it had been anecdotally relayed to the travel course faculty (TW) by students in years prior to this study that this ISL experience had greatly improved their clinical reasoning. Here we examined the scope and level of reflection by students writing individual reflection papers (RP) after a community engaged ISL program in Honduras.
Methods
Program Description
The ISL study abroad course was developed from a long-term (eight year) relationship between the primary author and local community leaders in Honduras to provide pro bono physical therapy services in an impoverished rural region of Honduras, where no such services exist.
Over the course of two years, 23 students across three cohorts enrolled in a cultural immersion study abroad ISL travel course led by the first author, offered as an elective through the Department of Physical Therapy. These three separate cohorts’ courses occurred during August 2018, October 2018 and August 2019. The October 2018 travel course had been rescheduled from December 2017 due to a travel advisory due to significant political unrest in Honduras following the disputed November 2017 elections. Course objectives focused on students developing an understanding of 1) typical struggles faced in the developing world (both material and non-material), 2) global health issues typically encountered, 3) how a multifaceted, evidence-based health promotion program with community participation, can positively modify the complex socioeconomic determinants of health, 4) and the ability to communicate effectively with others from another culture. The overarching purpose of the ISL travel course is to promote critical reflection and develop clinical reasoning via the clinical experience with cross-cultural dialogue, while broadening the students’ understanding of global citizenship [3].
Prior to departure, four 2-hour intensive pre-departure training class sessions were held, in addition to being given several assigned readings on the topics of ISL and global health issues. The in-country pro-bono clinic utilized a punctuated vertical mentoring model, where teams of two or three physical therapy students 1) perform a focused history to develop an initial clinical hypothesis, 2) then the physical exam, and finally 3) developed a clinical impression (assessment) and plan. Teams presented to a faculty physical therapist together at each stage for mentoring, feedback and direction. During the patient visit, wait times were used for a broad array of health education and promotion, linking patients with community resources and educating patients and family members on topics that included hypertension, obesity, nutrition and exercise. Each evening while in-country, students would gather for daily 360-degree cohort peer assessment feedback (assessments from others on the team) to discuss the cases and lived experiences of the day. The 360 feedback during the experience was implemented to maximize student learning and minimize ethical and safety risks [25, 26]. The in-country program included a 10-day immersion in Honduras in which students provided four days of supervised pro-bono outpatient physical therapy services in Taulabé set in a school setting, and one day of supervised pro-bono outpatient physical therapy services in Siquatepeque in a hospital setting (Hospital Evangélico). Students were encouraged to do daily individual journaling regarding their experiences that facilitate the writing of their RP. Sharing day-to-day experiences with one another helped to develop community amongst an already close group of students in each cohort. Students also were expected to explore the personal and professional impact of the ISL experiences; were mindful of how the experience would guide their future clinical practice, what world view perspective shifts occurred, and to what extend they hoped to “pay it forward”. These personal and professional impact elements were imbedded in their RP rubric, which they were provided prior to being in-country. Upon returning to the United States, students were required to complete the RP of 1500-2000 words within six weeks of return as their final assignment, guided by prompts based on Ash and Clayton’s [27] DEAL model for critical reflection (Figure 1).
Figure 1: Reflection Paper prompt based on Ash and Clayton’s [26] DEAL model for critical reflection.
Participants
For the purpose of this exploratory study, all 23 students were selected for analysis. Most (14/23) were female, and 22% (5/23) had never travelled outside of the US before. The study was approved by the institutional review board.
Assessment of Level of Reflection
A simplified four-category coding scheme initially developed by Kember et al.[28] from an earlier seven-category scheme (Kember, 1999) [29], and recommended for research needing to measure reflection as an outcome, was chosen as the protocol for assessment of level of reflection on the students RP assignment. In the scheme, the student’s written reflection is examined as a whole, and the global assessment of the level of reflective critical thinking is established by the highest level of reflection identified throughout the work. The four-level reflection scheme has been determined to have acceptable interrater reliability with a Cronbach’s a of .802 [30].
The following four levels of reflection categories [28] afforded parameters for assessing the level of reflective thinking demonstrated by each student.
- Non-Reflection/Habitual Action – no evidence of student attempting to reach an understanding of their experiences in relation to key concepts or values.
- Understanding – evidence of comprehension a concept identified, but the understanding does not relate to personal experiences.
- Reflection – circumstances encountered personally are considered in terms of values and personal insights.
- Critical Reflection – evidence of a change in perspective identified.
To maximize the reliability of Kember scores, all investigators participated in a facilitated discussion session on levels of reflection facilitated by members of a campus faculty development centre and completed reliability testing on three example reflection papers from a different ISL travel course that were not part of the sample.
Each participant’s paper was independently read and assessed on the Kember scale by two investigators (TE & JG), with the highest overall level of reflection demonstrated in the paper assigned to the participant per the recommended methods established by Kember et al. [28] Discrepancies in assigned Kember score were resolved by the third investigator (TW). In all, the scores of 5 participants (21.7%) were adjudicated by the third investigator.
Statistical Analysis
Descriptive statistics were calculated for participant demographics and Kember level of reflection (Table 1).Pearson’s chi-square test was used to determine if the proportion of individuals demonstrating Kember level 4 reflection differed between 1) females and males 2) those born before versus after the year 1994 (i.e. members of the “Millennial” versus “Generation Z” generations) and 3) years of the DPT curriculum completed. In the event that an analysis had one or more expected cell counts with a value less than 5, a Fisher’s exact test was used.
Results
The sample consisted of 14 females (60.9%) and 9 males. A total of 18 participants were born in or before 1994 (78.3%), and 5 were born after 1994. Seventeen participants had completed one year of the DPT curriculum (73.9%), and 6 had completed two. Kember scores ranged from 3 to 4, with a median and mode of 3. In all, 14 participants achieved a Kember level of 3 and 9 achieved a Kember level of 4. Sample demographics and Kember scores are in (Table 1).
| Participant Demographic Information | ||||||
| Kember Level 3 | Kember level 4 | Total | ||||
| Sex | n | % | n | % | n | % |
| Female | 7 | 30.4% | 7 | 30.4% | 14 | 60.9% |
| Male | 7 | 30.4% | 2 | 8.7% | 9 | 39.1% |
| Years in Curriculuma | n | % | ||||
| One | 11 | 47.8% | 6 | 26.1% | 17 | 73.9% |
| Two | 3 | 13.0% | 3 | 13.0% | 6 | 26.1% |
| Generationb | n | % | ||||
| Millennials | 11 | 47.8% | 7 | 30.4% | 18 | 78.3% |
| Generation Z | 3 | 13.0% | 2 | 8.7% | 5 | 21.7% |
| a. Represents number of years of DPT education completed | ||||||
| b. Millennials are those born between 1983 and 1994; Generation Z are those born after 1994 | ||||||
[/su_table]Table 1: Descriptive Statistics for Demographic Variables and Level of Reflection of Study Participants (N=23).
Due to expected cell counts less than 5 in each analysis, Fisher’s exact test was used to test for differences in the proportion of participants achieving Kember Level 4 reflection between the two levels of each explanatory variable. No statistically significant differences in proportion were found for any variable (sex p=0.23 years in curriculum p=0.64; generation p=0.99). Complete results are presented in (Table 2).
Results
Variable
Levels
p-Valuea
Sex
Female
Male
0.23
Years in Curriculumb
One
Two
0.64
Generationc
Millennial
Generation Z
0.99
a. Represents results of Fisher’s exact test
b. Represents number of years of DPT education completed
c. Millennials are those born between 1983 and 1994; Generation Z are those born after 1994
Discussion
This exploratory study investigated the level of critical reflection utilized by doctor of physical therapy students following an ISL travel course to Honduras using the 4-level Kember scale. No differences in reflection level were identified for any participant variable. We wanted to consider why the outcome measure (level of reflection) seen in the RPs was only at the level 3 and 4 categories. While indirect evidence, we believe a most reasonable explanation is that the course design of daily 360-feedback amongst peers and faculty while in-country, both through the structured punctuated vertical mentoring during patient encounters and during each day’s evening debriefing, engendered a level of trust not typically developed in a classroom setting. These exercises fostered a formative assessment process for the course content, and acted as a promoter of reflective meta-cognition process through the multifaceted lens of experiential, international, and intercultural learning. The trust cultivated during the time in-country, stimulates a reflective dialogue amongst students that promotes individual consideration of their encounters and experiences from alternative perspectives. Accordingly, RPs were more apt to indicate either a reflection regarding circumstances encountered through personal values or insights, or a change in perspective suggestive of a critical level of reflection that may have a bearing on their future physical therapy practice. For example, in a level 3 category score students might reflect that their view of the world expanded (or contracted) when they observe the dissimilar (or similar) struggles faced in a developing country. Alternatively, in a level 4 category score a student might critically reflect they are inspired to both live and practice as part of a community in order to best advocate for their patients, so that no one is underserved within that community.
Audette, Peterson and Svien [14] noted faculty to be motivated to use ISL because it “1) creates opportunities to shape the civic and moral dispositions of students, 2) serves as a positive model for teaching and learning, 3) provides an opportunity for students’ expression of personal identity, 4) can be an expression of institutional mission and values, and 5) fosters valuable community partnerships.” In addition to these factors, we advocate for the promotion of clinical reasoning. Ultimately, the intention of our ISL course designed reflection is improvement in clinical reasoning, as it is highly important in clinical education and professional development. Yet while it is essential, it is not a discrete measurable quantity and can prove difficult to measure. It should be noted that designing a quality assessment tool in the end may be an inefficient way to proceed in course development, rather spending time laying the groundwork for assessment (e.g. daily reflections, journaling, and 360-feedback). [22] There are multiple clinical reasoning assessment instruments that have been published in the literature. For example, the IDEA assessment tool is a 15-item instrument that asks assessors to rate medical students’ clinical skills of reporting, diagnostic reasoning, and decision-making skills based on medical students’ documentation of history and physical examination. The novel tool found moderate reliability for all three skill domains, including reporting skills (ICC = .53), diagnostic reasoning skills (ICC = .64), and decision-making skills (ICC = .63). [31] However, for health professions educators there are many others to choose from, as a recent scoping review (n=377) to identify the existing clinical reasoning measurement methods was performed, finding a plethora of tools that are applied across clinical, simulated clinical and non-clinical environments.[32]
Lessons Learned
It is well established that the use of reflection promotes the development of clinical reasoning [33]. Clinical reasoning is highly valued by the medical and rehabilitative professions, [34] and its utilization is therefore generally threaded throughout the curriculum at doctor of physical therapy education programs, often beginning in the first semester. Clinical reasoning is defined as a multidimensional process by which information, gathered together with the patient, is assessed to make decisions for diagnosis and treatment planning [35]. In medicine the most common clinical reasoning models for arriving at a diagnosis described in the medical literature are hypothetico-deductive reasoning (backward reasoning), utilized more frequently by the novice; and pattern recognition (forward reasoning), employed to a greater extend by the expert [36]. Regarding clinical reasoning in the physical therapy profession, Edwards et al. [37] offers one clinical reasoning approach for diagnosis and another for patient management. First, including the patient’s beliefs, experiences and cultures into the decision-making process (narrative reasoning), taken together with the formation of a movement-based classification predicated upon physical impairments while regarding tissue pathology, pain mechanisms, and other contributing factors (diagnostic reasoning) make up the strategy for diagnosis.
Secondly, patient management clinical reasoning strategies are further divided into six areas:
- Choosing and implementing an intervention (reasoning about procedure)
- Developing and maintaining patient rapport (interactive reasoning)
- Collaboration in all aspects of examination and plan of care (collaborative reasoning)
- Educating the patient in regards to their plan of care (reasoning about teaching)
- Consideration of future scenarios with patient (predictive reasoning)
- Consideration of the ethical implications of the clinical interventions (ethical reasoning)
We make the following recommendations for ourselves, and future like ISL travel courses that seek to develop clinical reasoning for their professional healthcare students (see Figure 2) as a student learning outcome for the course. 1. During and after initial patient encounters ask students to reflect on their clinical reasoning approach to diagnosis (e.g. narrative, diagnostic). 2. During and after patient encounters ask students to reflect on which of the reasoning strategies were utilized in patient care management. 3. Ask students to apply #1 and #2 within and across the WHO International Classification of Functioning, Disability and Health (ICF) model which describes functioning and disability in relation to a health condition [38]. For an extensive set of reflection questions for utilization during this patient-oriented clinical learning process, students are directed to the work of Atkinson and Nixon-Cave [39]. Providing reflection prompts that are patient focused will foster patient care reflective meta-cognition process apart from the larger ISL experience.
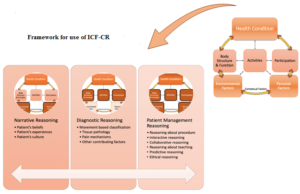
Figure 2: Illustration of integration of IFC clinical reasoning (ICF-CR) model in physical therapy for diagnosis and patient management applied through the lens of the International Classification of Functioning, Disability and Health. Dark brown cells indicate level of interaction of clinical reasoning with the ICF-CR model. Figure adapted from World Health Organization. Towards a common language for functioning, disability and health: ICF, the international classification of functioning, disability and health. http://www.who.int/classifications/icf/training/icfbeginnersguide.pdf. Published 2002. [37].
Limitations
Study limitations included the use of an underpowered, convenience sample of participants who were not matched for gender, generation or education characteristics. While the program was conducted by the same professor in the same community in Honduras, variations in ISL travel course experience were bound to occur between groups in terms of individual patient encounters. Recommendations for future studies are increasing the number of participants for sufficient random allocation into groups yielding adequate statistical power and inclusion of RP prompts directed towards patient care processes.
Conclusion
This exploratory study found DPT student RP regarding their ISL travel course experience to be written at the highest (reflective and critically reflective) Kember scale levels. No differences in levels of reflection were identified for age, gender or years in the DPT program. It is possible that the nature of the daily feedback sessions among students and faculty during patient encounters and daily evening briefing sessions promoted a culture of trust, self-awareness and critical reflection for all students not typical of a traditional classroom environment. Recommendations are made for future use of reflection prompts geared toward clinical reasoning throughout patient care within the framework of the WHO ICF model. Ultimately, the ISL travel course achieved its goal of fostering critical reflection to enhance the quality of the clinical experience and cross-cultural dialogue, while broadening the students’ understanding of global citizenship.
References
- Nixon SA, Hunt M (2015) Global Health: Where Do Physiotherapy and Rehabilitation Research Fit?. Physiother Canada 67: 217-218.
- APTA (2016) International service manual for students. www.apta.org.
- Bringle RG, Hatcher JA, Jones SG (2011) International service learning: conceptual frameworks and research. 78-82.
- Butin DW (2010) Service-Learning in Theory and Practice. New York: Palgrave Macmillan US.
- Ikeda E, Sandy M, Donahue D (2010) Navigating the sea of definitions. In: Looking in Reaching out: A Reflective Guide for Community Service-Learning Professionals 17-29.
- Jacoby B (2015) Service-Learning Essentials: Questions, Answers, and Lessons Learned. 1st ed. San Francisco, CA: Jossey-Bass.
- Bringle R, Hatcher J (2002) Campus-community partnerships: the terms of engagement. J Soc Issues 58:503-516.
- Soska TM, Sullivan-Cosetti M, Pasupuleti S (2010)Service Learning: Community Engagement and Partnership for Integrating Teaching, Research, and Service. J Community Pract 18:139-147.
- Witherell S, Clayton E(2014) Institute of International Education (New York NY) Open Doors 2014 : Report on International Educational Exchange.
- European Commission (2014) The Erasmus Impact Study.
- Mawji A, Lind C, Loewen S, Underwood M, Thompson-Isherwood R (2014) “Slapped In the Face with It”: Internalizing Community Health Concepts from an International Practice Setting. Int J ApplSci 4:29-36.
- Raterink G (2016) Reflective Journaling for Critical Thinking Development in Advanced Practice Registered Nurse Students. J NursEduc 55: 101-104.
- Pechak CM, Black JD (2014) Exploring international clinical education in US-based programs: identifying common practices and modifying an existing conceptual model of international service-learning. Physiother Theory Pract 30: 94-104.
- Audette J, Peterson C, Svien L(2018) Toward Optimizing Global Learning Opportunities for US Physical Therapy Students: A Description of Current Practices and Initial Recommendations. J PhysTherEduc 32:77-86.
- Audette JG, Roush SE (2013) Educational Perspectives and Teaching Styles of Faculty Who Lead International Service-Learning Experiences: J PhysTherEduc 27: 65-73.
- Pechak CM, Thompson M (2009) A conceptual model of optimal international service-learning and its application to global health initiatives in rehabilitation. PhysTher 89: 1192-1204.
- Mezirow J (1998) On Critical Reflection. Adult Educ Q 48:185-198.
- Gargallo B (1993) Basic variables in reflection-impulsivity : a training programme to increase reflectivity. Eur J PsycholEduc 8: 151-167.
- Powell JH (1989) The reflective practitioner in nursing. J AdvNurs 14: 824-832.
- Richardson G, Maltby H (1995) Reflection-on-practice: enhancing student learning. J AdvNurs 22: 235-242.
- Perry L, Stoner L, Tarrant M(2012)More Than a Vacation: Short-Term Study Abroad as a Critically Reflective, Transformative Learning Experience. CreatEduc 3: 679-683.
- Deardorff DK (2015) Demystifying Outcomes Assessment for International Educators: A Practical Approach. Sterling, Virginia: Stylus Publishing 74: 197-199.
- Klaeson K, Berglund M, Gustavsson S (2016) The character of nursing students’ critical reflection at the end of their education. J NursEducPract 7: 55-61.
- Schuessler JB, Wilder B, Byrd LW (2012) Reflective Journaling and Development of Cultural Humility in Students. NursEducPerspect 33: 96-99.
- Dell EM, Varpio L, Petrosoniak A, Gajaria A, McMcarthy AE (2014) The ethics and safety of medical student global health electives. Int J Med Educ 5: 63-72.
- Rhodes G (2019) International Travel Safety in Perspective Balancing Safety Issues While Supporting Study Abroad Program Implementation. Accessed November 25, 2019.
- Ash SL, Clayton PH (2009) Generating, Deepening, and Documenting Learning: The Power of Critical Reflection in Applied Learning. J Appl Learn High Educ1:25-48.
- Kember D, McKay J, Sinclair K, Wong FKY (2008) A Four-Category Scheme for Coding and Assessing the Level of Reflection in Written Work. Assess Eval High Educ 33: 369-379.
- Kember D, Jones A, Loke A, Jan M, Kit S, et al. (1999) Determining the level of reflective thinking from students’ written journals using a coding scheme based on the work of Mezirow. Int J LIFELONG Educ18: 18-30.
- Bell A, Kelton J, McDonagh N, Morrison K, Mladenovic R (2011) A critical evaluation of the usefulness of a coding scheme to categorize levels of reflective thinking. Assess Eval High Educ 36: 797-815.
- Baker EA, Ledford CH, Fogg L, Way DP, Park YS (2015) The IDEA Assessment Tool: Assessing the Reporting, Diagnostic Reasoning, and Decision-Making Skills Demonstrated in Medical Students’ Hospital Admission Notes. Teach Learn Med 27: 163-173.
- Daniel M, Rencic J, Durning SJ, Holmboe E, Santen SA, et al. (2019)Clinical Reasoning Assessment Methods: A Scoping Review and Practical Guidance. Acad Med 94: 902-912.
- Murphy JI (2004) Using focused reflection and articulation to promote clinical reasoning: an evidence-based teaching strategy. NursEducPerspect 25: 226-231.
- Higgs Joy, Jones MA, Loftus Stephen, Christensen Nicole, Higgs Joy (2014) Clinical Reasoning in the Health Professions.
- Jensen GM, Gwyer J, Shepard KF (2000) Expert practice in physical therapy. PhysTher80:28-43; discussion 44-52.
- Elstein AS, Shulman LS, Sprafka SA (1978) Medical Problem Solving: An Analysis Clinical Reasoning. Cambridge, Mass.: Harvard University Press.
- Edwards I, Jones M, Carr J, Braunack-Mayer A, Jensen GM (2004) Clinical reasoning strategies in physical therapy. Phys Ther 84:312-330; discussion 331-335.
- World Health Organization. (2002) towards a common language for functioning, disability and health: ICF, the international classification of functioning, disability and health.
- Atkinson HL, Nixon-Cave K (2011) A tool for clinical reasoning and reflection using the international classification of functioning, disability and health (ICF) framework and patient management model. PhysTher 91: 416-430.