Publication Information
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Cybersickness Associated with Participating in an International Virtual Reality-Style Conference
Masafumi Sakashita MD, PhD a, 1, Nozomu Takata PhD b, c, 1, Masayuki Okamoto MD, PhD a, Myungmi Oh MD, PhD a, Yukihiro Kimura MD, PhD a, Takahiro Tokunaga MD, PhD a, d, Akimi Oyanagi, PhD e, Eri Kubota, MBA f, Tomohiro Amemiya, PhD e, Shigeharu Fujieda MD, PhD a, Takeya Adachi MD, PhD c, g, h, i, *
aDepartment of Otorhinolaryngology Head and Neck Surgery, University of Fukui, 23-3 Shimoaizuki Eiheiji-cho Matsuoka, Yoshida-gun, Fukuji, 910-1193 Japan.
bCenter for Vascular and Developmental Biology, Feinberg Cardiovascular and Renal Research Institute, Northwestern University Feinberg School of Medicine, 303 East Superior Street, Chicago, Illinois 60611 USA.
cUnited Japanese Researchers Around the world (UJA)
dOtorhinolaryngology, Shinseikai Toyama Hospital, 89-10 Shimowaka, Imizu, Toyama, 939-0243 Japan
eVirtual Reality Educational Research Center, The University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo, 113-8656 Japan
fMediproduce Inc, Ebisu #B5, Glass Square, Yebisu Garden Place 4-20-4 Ebisu, Shibuya-Ku, Tokyo, 150-6090 Japan
gDepartment of Medical Innovation and Translational Medical Science, Graduate School of Medical Science, Kyoto Prefectural University of Medicine; Kawaramachi-Hirokoji, Kajii-cho, Kamigyo-ku, Kyoto-shi, Kyoto, 602-8566 Japan
hKeio Frontier Research & Education Collaborative Square (K-FRECS), Keio University, 3-25-10 Tonomachi, Kawasaki-ku, Kawasaki-shi, Kanagawa, 210-0821 Japan
iDepartment of Dermatology, Keio University School of Medicine, 35 Shinanomachi, Shinjuku City, Tokyo 160-8582 Japan.
1These authors contributed equally to this work.
Received Date: July 08, 2024; Accepted Date: August 11, 2024; Published Date: October 17, 2024;
*Corresponding author: Takeya Adachi, MD, PhD; Department of Medical Innovation and Translational Medical Science, Graduate School of Medical Science, Kyoto Prefectural University of Medicine, Kyoto, Japan 465 Kajii-cho, Kawaramachi-Hirokoji, Kamigyo-ku, Kyoto 602-8566, Japan; Department of Dermatology, Keio University School of Medicine 35 Shinanomachi, Shinjuku-ku Tokyo 160-8582 JAPAN Tel: +81-3-5363-1211 E-mail: jpn4156@me.com
Citation: Sakashita M, Takata N, Okamoto M, Myungmi OH, Kimura Y, Tokunaga T, Oyanagi A, Kubota E, Amemiya T, Fujieda S, Adachi T (2024) Cybersickness Associated with Participating in an International Virtual Reality-Style Conference – Head and Neck: AOHNS-115.
DOI: 10.37722/AOHNS.2024202
Abstract
Recent technological advances have increased the use and application of virtual reality tools. However, the health hazards associated with these tools in the real world have not been investigated especially in an international scientific conference. Therefore, this study aims to clarify the characteristics of cybersickness, a typical side effect of virtual reality. A web-based questionnaire written in Japanese was distributed to 69 participants of a virtual reality-style conference. Among the 69 respondents (response rate of 33%; 46 participants from Asia and 23 from Europe and the United States) who completed all required items, eight experienced symptoms of cybersickness. These symptoms frequently occurred during the first hour of participation (62.5%). Moreover, the participants with head-mounted displays experienced cybersickness (p = 0.03). Two participants (4.3%) from Asia developed cybersickness during the daytime; however, six participants from Europe and the United States experienced cybersickness during the night time, suggesting that a significant chance of cybersickness existed for people who participated in the conference at night (p = 0.01). Cybersickness while attending the virtual reality-style conference frequently occurred in countries with different time zones. Our findings highlight the necessity of identifying the major factors that cause virtual reality related conflicting signals in the brain to formulate strategies for reducing symptoms of cybersickness during advanced communication technologies.
Keywords: Cybersickness, virtual reality, head-mounted displays, sensory conflicts, time zone
Introduction
The spread of severe acute respiratory syndrome coronavirus 2 has resulted in restrictions and reduced the need for interpersonal communication. Consequently, online videoconferencing tools for non-contact conferences and meetings have increased dramatically (Karl et al. 2022). Remote communications are not restricted by physical and spatial constraints; however, they would not provide the same sense of presence and realism as that experienced in physical spaces (Greenwald etal. 2017). Virtual reality (VR) technology has become a popular application for creating “VR environments for play” since the 1970s, owing to the rapid advancement of computer graphics and other visual information technologies (Gigante 1993). VR has been a growing and attractive technology that facilitates social interactions in three-dimensional (3D) spaces using artificial intelligence. The Web of Science statistics on VR by category has highlighted that computer science, rehabilitation, education, and clinical neurology are four of the top 10 studies (Gigante 1993). Interestingly, VR or Metaverse applications have been developed commercially and economically, and they have garnered increased attention. This trend has been further highlighted by the active pursuit of Metaverse realization by Facebook, a global social network company (Rodriguez 2021).
Development of inexpensive and user-friendly devices is expected to expand the range of VR applications. However, immersion in an environment different from the previous one would pose the risk of new health hazards. This is likely because VR is negatively associated with the experience of “presence” in virtual space and can cause disorders affecting human health (Weech et al. 2019). Cybersickness (VR sickness), a syndrome that occurs in the absence of physical motion, is similar to motion sickness (Gavgani et al. 1985). Additionally, VR sickness can cause discomfort and various symptoms such as nausea, headache, dizziness, fatigue, and eyestrain (Keshavarz et al. 2023). Therefore, cybersickness can alter the future spread of VR technologies, and these pieces of evidence suggest addressing its safety concerns is crucial before it escalates into a global issue.
Motion sickness is a physiological response characterized by dizziness, which is a normal reaction to an abnormal situation. The condition is triggered by certain types of motion; it can be induced by an unfamiliar physical acceleration to which one has not adapted during passive movement in a vehicle, or by an intersensory conflict between vestibular and visual stimuli (Schmäl 2013). Previous research has revealed that sensory conflict theory is the most promising hypothesis for the cause of motion sickness (Reason 1978). Furthermore, three subtypes of sensory conflicts exist. Type 1 occurs when visual and vestibular receptors simultaneously signal motion but lack correlation or compatibility. Examples include swinging on playground equipment in amusement parks while observing the movement of the surrounding scenery. Type 2 occurs when the visual receptors perceive a relative motion of large portions of the visual field. Normally, visual and vestibular stimulations signal head and body movements; however, vestibular movements are absent in Type 2 conflicts. One example of Type 2 motion sickness, also known as simulator sickness, is the sensory confusion that occurs while operating simulators in driving schools. Sensory confusion is caused by the difference between driving in a simulator and the real world (Crowley 1987; Dużmańska et al. 2018). In a Type 3 conflict, a vestibular stimulus is present; however, a correlated visual stimulus is absent, corresponding to motion sickness caused by reading while riding in a vehicle. Most cybersickness cases are classified as Type 2 sensory confusion. Recently, although opportunities to use VR, 3D computer graphics (CG), and two-dimensional (2D) tools have increased considerably, their health hazards in the real world have not been investigated. Therefore, this study aims to clarify the characteristics of cybersickness, a typical side effect of VR.
2. Materials and Methods
2.1 Study design
The principal investigator conducted this survey to study cybersickness, such as dizziness caused by VR, in a forum that used cross-reality technologies to improve the experience and communication between physical and digital environments (Japan XR Science Forum 2020, July 11, 2020. https://www.japanxr-science-forum.org). The University of Fukui Ethical Review Committee (approval number: 20200062) approved this study, and a virtual medical office with otolaryngologists was established to ensure the safety of participants. Of the 1,117 participants, we conducted a sampling survey of 211 randomly selected participants, maintaining a 2:1 ratio by country. Of the responses obtained, we analyzed data from 69 participants (response rate of 33%; 46 participants from Asia and 23 from Europe and the United States) who completed all the required items. These participants received a questionnaire via Survey Monkey (https://www.surveymonkey.com), an online survey tool, between July 12, 2020, and July 31, 2020. Anonymous respondents were recruited in Japan through invitations sent to registered email addresses and Slack (a collaborative tool used for communication among participants). Data regarding nationality was not collected during the survey. We assumed that the participants were either Japanese or its native speakers because the event was mainly conducted in Japanese language. All data with the completed required items were analyzed.
2.1.1 Consent of participants, and patient and public involvement
The consent of participants to use their data in analytical studies for publication was obtained electronically. According to the study design, registrants with a medical history of vertigo or dizziness were asked to participate. In addition, we invited otolaryngologists from the University of Fukui to a virtual medical office to regularly monitor the participants with symptoms during the conference. One registrant and two otolaryngologists prepared the final questionnaire.
2.1.2 Conference programs
Various programs were reconstructed in the VR space at each venue during the daytime setting, including award presentation ceremonies by avatars, talks about studying abroad, parent-child science classes, oral or poster research presentations, exchange programs for joint research among different fields, company exhibitions, book sales, and luncheon seminars. Additionally, VR Chat (https://hello.vrchat.com/), hubs (https://hubs.mozilla.com/), Zoom, and YouTube were also available (see press releases before and after the forum) (Okada 2020).
2.1.3 Participants
VR Chat, a 3D CG tool with an HMD, and Hubs, a 3D CG tool without an HMD, allowed the participants to control and move their avatars with a sense of physical movement (Schmäl 2013).
HMDs used in VR Chat included VIVE
(https://www.vive.com/us/), Oculus Rift
(https://www.oculus.com/rift/),
Google Cardboard (https://arvr.google.com/cardboard/),
and Oculus Quest (https://www.oculus.com/quest/refurbished/).
However, online 2D tools (Zoom/YouTube Live) only allowed participants to view the virtual space on the screen and did not require a sense of physical movement. Furthermore, owing to the nature of the program, the transition from 2D to 3D and vice versa was not specifically investigated.
The main conference programs and devices used were as follows:
- Ceremony at the main venue: VR Chat with Windows and head-mounted gears
- Hubs poster sessions: Windows or Mac personal computers, tablets, or smartphones
- Zoom A/B venues: Windows or Mac personal computers, tablets, or smartphones
- YouTube venue: Windows or Mac personal computers, tablets, or smartphones
2.1.4 Demographics of participants
In the first section, a survey was conducted considering age, sex, region, and time of participation. The participating countries included Japan, Singapore, France, and the United States. Participation time was divided into 30-minute intervals, with options ranging from ≤30 minutes to ≥5 hours. The conference program was conducted in the morning in Asian countries and at night in the United States and Europe (midnight).
2.2. Clinical assessment
We investigated the presence or absence of VR experiences and the number of previous VR experiences (Table S1). First, the participants were asked to provide details of the electronic devices used for participation and whether they were smartphones, tablets, or personal computers with or without HMDs. Second, we asked the participants about their physical condition, whether they had motion sickness, which symptoms appeared during the program, and the duration of the symptoms. Third, participants with a history of dizziness were noted. Fourth, we inquired if the participants had previously experienced motion sickness (vehicles, including public transportation, such as trains, buses, airplanes, and amusement rides, such as boats and swings in playgrounds). Additionally, we inquired whether the symptoms above were experienced before, during, or after participation. This information was used to determine the validity of the survey data. If the symptoms were experienced during participation, the survey was divided into 30-minute intervals, with options ranging from ≤30 minutes to ≥5 hours. Participants identified the program in a selective format (first half of the ceremony, cell x latest research, interdisciplinary exchange x post-study career, poster session, and second half) where their symptoms mainly appeared.
2.3. Statistical analyses
Examining the ratio of cybersickness occurrence between the groups, the population ratio and 95% CIs were estimated and compared using Fisher’s exact probability test. Statistical significance (p) was set at 0.05. Statistical analysis was conducted using Statcel4 software (OMS Publishing Ltd. Tokyo, Japan).
3. Results
3.1. Demographics of participants
A web-based questionnaire written in Japanese (Supplemental Table 1) was distributed to randomly selected participants (Fig. 1a). Participants who attended the conference were recruited by members of the United Japanese Researchers Around the World. Of the 1,117 participants, 211 were randomly selected and 69 completed the questionnaire (46 males and 23 females, 32.7% response rate). The question “Did you experience any dizziness or unusual sensations during the meeting?” was answered “No” by 61 people; however, eight respondents answered “Yes” and were inferred as experiencing cybersickness in this study. The office of a doctor was available in case of any emergency; however, none of the eight patients reported any serious health issues. Eight participants experienced symptoms of cybersickness (Fig. 1b). Five out of 46 respondents were male (10.9%) and three out of 23 were female (13.0%). Regarding the age group of participants with cybersickness symptoms, one out of three (33.3%) were in their 20s, three out of 19 (15.7%) were in their 30s, three out of 20 (15.0%) were in their 40s, and one out of 12 (8.3%) was in his/her 50s.
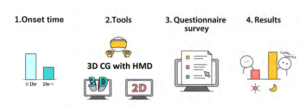
Figure 1a: Overview of the method used for investigating the occurrence of cybersickness during virtual reality (VR) conferences
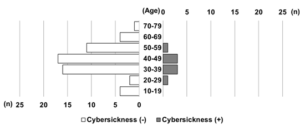
Figure 1b: Cybersickness cases by age group
The vertical axis represents the number of people in each age group who participated in the VR conference and answered the questionnaire. On the horizontal axis, the gray and white bars indicate the number of people (n) who developed or did not develop cybersickness, respectively (n).
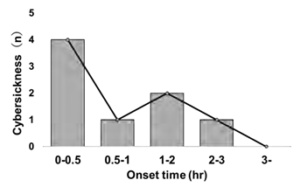
Figure 2: Elapsed time from participation in the virtual reality (VR) conference to the onset of cybersickness
The vertical axis represents the number of people who developed cybersickness at each time point (n) and the horizontal axis represents the elapsed time from participation in the VR conference to the onset of cybersickness.
3.2. Relationship between onset time, participation program, and cybersickness
More than half of the participants (five out of eight, 62.5%) experienced cybersickness within the first hour of participation (Fig. 2). Table S2 contains information about the number of people and the time of day when they developed cybersickness. Five participants (one from Japan and four from the United States) experienced cybersickness with sensations of body movement within the first hour of a 3D event (opening ceremony; Table 1). However, three participants (one from Japan and two from the United States) experienced cybersickness within the first hour, even during the 2D event where no bodily movement sensation was involved (with session titled “cells × the latest research interdisciplinary exchange”). All participants experienced symptoms of cybersickness during the conference with no pre-participation dizziness or unusual sensations. In contrast, no cybersickness was observed during the 2D event after more than 2 hours of participation. However, two people developed cybersickness during the 3D event after more than 2 hours of participation.
Table 1. Content of the conference at the time of onset
| Contents | Event* | JST | Cybersickness (n) | CST | Cybersickness (n) | with HMD (n) |
| Opening Ceremony | 3D | 7:00 am | 1 | 5:00 pm | 2 | 2 |
| Cells X The latest research | 2D | 7:50 am | 1 | 5:50 pm | 2 | 1 |
| Interdisciplinary exchange X Carrier after studying abroad | 2D | 9:20 am | 0 | 7:20 pm | 0 | 0 |
| Poster tours and session | 3D | 10:50 am | 0 | 8:50 pm | 2 | 0 |
| Closing Ceremony | 2D | 11:20 am | 0 | 9:20 pm | 0 | 0 |
2D, two dimensional; 3D, three dimensional; HMD, head mounted display; JST, Japan Standard Time; CST, Central Standard Time
*2D and 3D indicate the visual dimensions of each event.
3.3. Relationship between the device used for participation and cybersickness
Three (42.9%) of the seven participants who used head-mounted displays (HMDs) experienced cybersickness (95% confidence interval [CI, 15.7–75.0]) (Table 2). Overall, five (8.1%) of the 62 participants who did not use HMDs experienced cybersickness (95% CI [3.1–17.9]). The occurrence of dizziness was significantly high in the group using HMDs for personal computer use (p = 0.03); however, no cybersickness was observed in the Zoom and YouTube Live groups. Table 1 presents the program details, visual dimensions, local times in Japan, Singapore, the United States, and France; the number of patients with cybersickness; and the use of HMDs.
Table 2. Usage of HMD
| Total (n) | Cybersickness (n) | Proportion (%) | [95 % CI] | P value | |
| With HMD | 7 | 3 | 42.9 | [15.8-75.00] | 0.03 |
| Without HMD | 62 | 5 | 8.1 | [3.1-17.9] |
[s/u_table]HMD, head-mounted displays; CI, confidence interval.
3.4. Relationship between local time and cybersickness
At the conference, 45 and 22 participants were from Japan and the United States, respectively. Additionally, one participant was from France and another was from Singapore. The VR conference was held at 7:00 am in Japan and at 9:00 pm in the United States (Central Standard Time) to allow more countries to participate. Two people from Japan and six from the United States experienced cybersickness. The estimated population ratio of participants from Asia, including Japan and Singapore that developed cybersickness was 4.3% (two out of 46), 95% CI (0.4–15.3), and those from the United States and France who experienced cybersickness was 26.1% (six out of 23), 95% CI (12.3−46.8), p = 0.01 (Fig. 3a). No difference in the participation rates was observed between the two groups with respect to the 2D and 3D visual dimensions (Fig. 3b). More participants from the United States developed cybersickness than those from other countries. This indicates that VR participation at night may have a greater impact on cybersickness than participation during the day.
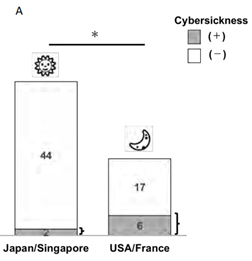
Figure 3a: Relationship between local participation time and the onset of cybersickness
The incidence of cybersickness was compared between Japan and Singapore (participation from 7:00 a.m.) and the United States and France (participation from 9:00 p.m.). The gray and white bars indicate the number of people (n) who developed or did not develop cybersickness, respectively. *p < 0.01
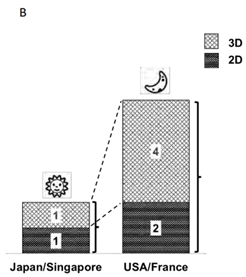
Figure 3b: Relationship between the participating events and onset of cybersickness
The number of participants in two-dimensional (2D) and three-dimensional (3D) events among two Japanese and six United States participants who developed cybersickness. The black bars represent 2D events and the shaded bars represent 3D events.
3.5. Relationship between VR experience, history of dizziness and vertigo disorders, history of motion sickness, and cybersickness
Four patients with cybersickness experienced VR for the first time at this conference (Table 3). The other four patients with cybersickness had prior experience with VR. These results suggest that the number of past VR experiences may not prevent cybersickness experienced at VR conferences.
Approximately two (13.3%) of the 15 participants with a history of dizziness and vertigo disorder developed cybersickness. However, six (11.1%) of the 54 participants without a history of dizziness or vertigo experienced cybersickness (Table 4). No significant relationship was observed between the occurrence of cybersickness and a history of dizziness or vertigo. Of the 32 participants who reported being prone to motion sickness, four (12.5%) experienced cybersickness. Additionally, four (11.1%) of the 36 participants who were not prone to motion sickness experienced cybersickness
Table 3: Number of VR experiments
| Number of VR experiences | All participants (n) | Cybersickness (n) | Proportion (%) | [95% CI] | P value |
| Non-participation | 16 | 0 | 0 | [-3.3-22.7] | NS |
| 1st Time | 35 | 4 | 11.4 | [3.9-26.5] | NS |
| 2nd–5th times | 9 | 2 | 22.2 | [5.3-55.7] | NS |
| 6th–10th times | 3 | 1 | 33.3 | [5.6-79.8] | NS |
| 11th times or more | 6 | 1 | 16.7 | [1.1-58.2] | NS |
VR, virtual reality; CI, confidence interval.
Table 4: Relationship between symptoms and vertigo disorder and motion sickness
| History | All participants (n) | Cybersickness (n) | Proportion (%) | [95% CI] | P value | |
| Vertigo diseases | Yes
No |
15
54 |
2
6 |
13.3
11.1 |
[2.5-39.1]
[4.3-22.6] |
NS |
| Motion sickness | Yes
No |
32
36 |
4
4 |
12.5
11.1 |
[4.4-28.8]
[3.8-25.9] |
NS |
4. Discussion and Conclusion
4.1. Discussion
Following the outbreak of the 2019 coronavirus pandemic, approximately all international conferences, including specialized academic conferences such as The Institute of Electrical and Electronics Engineers Conference on VR and 3D User Interfaces, have been conducted virtually using video-conferencing tools (IEEE Computer Society 2022). The proliferation of interactive discussions on VR exchange platforms is expected to popularize VR conferences. However, the increase in cybersickness is a major cause for health concern. Therefore, verifying whether the VR platforms are capable of hosting international conferences is necessary. Few cross-sectional surveys of cybersickness have been conducted in the real world, such as those at large-scale conferences. We directly compared the differences in the participation time, devices, local time, and medical history of dizziness while sharing the VR experience. We discovered that the onset of cybersickness frequently occurred within 1 hour of participation. The participants using HMDs often experienced cybersickness. Cybersickness symptoms occurred irrespective of age, number of VR experiences, or history of dizziness or motion sickness. In addition, participation at night in VR conferences may influence the onset of cybersickness.
Certain aspects of VR programs, such as hardware and software latency, can affect cybersickness (Chessa et al. 2019; Howarth and Costello 1997; Kennedy et al. 2010; Sharples et al. 2008). Sensory conflict theory is one of the leading hypotheses about the causes of motion sickness (Schmäl 2013). Moreover, Type 2 cybersickness is characterized by sensory confusion in which visual information is present, but vestibular and somatosensory information is absent. The discrepancy between regulatory and convergent information caused by HMDs contributes to the cybersickness experienced with the use of VR devices (McCauley and Sharkey 1992). In this study, no relationship was observed between the history of VR experience and the onset of cybersickness. Additionally, VR sickness intensifies as the sense of realism increases while using a driving simulator in a virtual environment (Lin et al. 2022). In our study, cybersickness was predominantly observed among participants using HMDs, consistent with previous observations (Lin et al. 2022).
We observed that cybersickness was likely to occur within the first hour of participation in VR-style conferences, and it was unaffected by the length of stay of the participant. Kennedy et al. (Kennedy et al. 2000) discovered a deceleration in the decline of simulator sickness severity over time in a study involving military pilots who participated in seven consecutive helicopter simulator training sessions. Repeated-measures analysis revealed a monotonic decrease in the severity of simulator sickness as a function of the flight number. They proposed that short, repeated simulator exposures may be used to achieve cybersickness adaptation (Kennedy et al. 2000). However, the effects of local time on hardware and software factors as well as the individual differences have not been examined in recent studies. We discovered that the use of HMD was likely to cause cybersickness when the participation was at night owing to the time zone difference. The bright VR environment may have induced a shift in sensation contrary to the sense of night perceived by the VR participants in the real environment. Vestibular dizziness frequently affects doctors and nurses working at night than those working during the day (Bashir et al. 2020). Melatonin is suppressed during night shifts by high luminance (Nagashima et al. 2018; Hartstein et al. 2022). In our study, the presence or absence of a history of dizziness was not identified as a risk factor for cybersickness. Therefore, the observed differences are likely attributable to variations in time zones. In future VR conferences, we recommend that participants should be educated about cybersickness during the first hour, especially those participating at night.
Among the individual factors that cause vertigo, dizziness is more common in older adults, because vestibular function declines with age. For example, the prevalence of vestibular dizziness was 3% in the 18–29-year age group but increased to 8.8% in the 70-year age group (Neuhauser et al. 2005). Cybersickness is less likely to occur in older adults with reduced vestibular function because its mechanism involves a mismatch between visual and vestibular or somatic information; however, these reports are controversial (Saredakis et al. 2020; Arns and Cerney 2005).
4.2. Limitations
We observed intriguing possibilities for medical considerations when participating in VR meetings during the 2020 pandemic. However, the research registrants in this study may not fully reflect the characteristics of the original population because only 69 of the 211 registrants fully answered the surveys. Furthermore, the number of participants who used HMDs was lower than expected, partly because of the difficulty and cost associated with handling systems featuring HMDs for scientists attending VR conferences for the first time. We cannot rule out racial differences in this survey; however, most participants were Japanese with similar genetic makeup. Furthermore, we did not use subjective evaluation methods such as those used by Graybiel et al. (1968) to determine the level diagnosis classification for motion sickness or Kennedy et al.(1993) simulator sickness questionnaire for quantifying simulator and virtual environment sickness.
We did not inquire about several factors in the questionnaire, including head movement while moving, engagement in tasks, attention to viewpoints, or posture (Webb and Griffin 2002; Griffin and Newman 2004). Drugs, such as antihistamines, parasympathetic blocking agents, and central nervous system stimulants, can prevent motion sickness (Gahlinger 1999; Sherman 2002). This study included only five participants (7.2% of the total) who were aged ≥ 60 years; therefore, future studies on a large number of older patients are recommended. We were unable to collect this information in our study; therefore, we recommend consideration of the aforementioned information in future research. Other studies have indicated that individual differences among users, such as sex and age, may help predict cybersickness (Munafo et al. 2017; Tyrrell et al. 2018; Zhang et al. 2016). Insomnia and postural stability are related to simulator sickness (Altena et al. 2019). However, this study did not collect data on insomnia or postural stability. Furthermore, some individuals may not have responded to the survey owing to them being unaffected by cybersickness. This study did not rule out the possibility that cybersickness varies between night and day. This preventive warning is necessary for the safe use of VR platforms. Therefore, we emphasize the importance of preventive research and development that matches the time zone of the user and the VR brightness of the background.
4.3. Conclusion
Cybersickness was mostly observed when 3D tools were used and within the first hour of participation in VR events. In addition, cybersickness is more likely to occur when the participants use VR platforms at night. Age, number of VR experiences, history of vertigo disorders, or motion sickness did not affect the occurrence of cybersickness. When conducting future VR conferences, measures to prevent cybersickness should be considered for the well-being and safety of the participants.
Statements and Declarations
Competing interests: None.
Funding: This work was supported by the Scientific Research Fund of the Ministry of Health, Labor, and Welfare, Japan (21FE2001) to Tad; and the UNION Foundation for Ergo Design Culture Funding (3-123) to EK.
Data availability statement: The data that support the findings of this study are available on request from the corresponding author, TA. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Compliance with Ethical Standards
Research involving human participants: Not applicable.
Informed consent: The consent of participants to use their data in analytical studies for publication was obtained electronically.
Author Contribution: MS and NT contributed equally to this work. MS and NT contributed substantially to the conception and design, as well as the acquisition, analysis, and interpretation of data. MS and NT also drafted and critically revised the manuscript. MS, MO, MO, YK and TT contributed data collection, data curation, formal analysis and visualization. AO, TA contributed to methodology and resource. EK contributed funding acquisition for database construction. TA contributed to project administration, writing – review and editing. SF contributed to supervision. All authors discussed the results and commented on the manuscript.
References
- Karl, A., Peluchette, J.V., Aghakhani, N., 2022. Virtual work meetings during the COVID-19 pandemic: the good, bad, and ugly. Small Group Res. 53, 343–365. https://doi.org/10.1177/10464964211015286.
- Greenwald, W., Wang, Z., Funk, M., Maes, P., 2017. Investigating Social Presence and Communication with Embodied Avatars in Room-Scale Virtual Reality, in: Dr. Beck, D., Dr. Allison, C., Morgado L., et al, Immersive Learning Research Network. iLRN. Communications in Computer and Information Science, vol 725. Springer, Cham, pp. 75–90. https://doi.org/10.1007/978-3-319-60633-0_7
- Gigante, A.,1993. Virtual reality: definitions, history and applications. Virtual Reality Systems, in: Earnshaw, R.A., Gigante, M.A., Jones, H. (Eds.), Virtual Reality Systems. Academic Press, pp. 3–14. https://doi.org/10.1016/B978-0-12-227748-1.50009-3
- Cipresso, , Giglioli, I.A.C., Raya, M.A., Riva, G., 2018. The Past, Present, and Future of Virtual and Augmented Reality Research: A Network and Cluster Analysis of the Literature. Front. Psychol. 9, 2086. https://doi.org/10.3389/fpsyg.2018.02086
- Rodriguez , 2021. Facebook takes a step toward building the metaverse, opens virtual world app to everyone in U.S. https://www.cnbc.com/2021/12/09/facebook-opens-horizon-worlds-vr-metaverse-app-.html (accessed 21 January 2022).
- Weech, , Kenny, S., Barnett-Cowan, M., 2019. Presence and Cybersickness in Virtual Reality Are Negatively Related: A Review. Front. Psychol. 10, 158. https://doi.org/10.3389/fpsyg.2019.00158
- Gavgani, A., Walker, F.R., Hodgson, D.M., Nalivaiko, E., 1985. A comparative study of cybersickness during exposure to virtual reality and “classic” motion sickness: are they different. J. Appl. Physiol. 125, 1670–1680. https://doi.org/10.1152/japplphysiol.00338.2018
- Keshavarz, , Murovec, B., Mohanathas, N., Golding, J.F., 2021. The Visually Induced Motion Sickness Susceptibility Questionnaire (VIMSSQ): Estimating Individual Susceptibility to Motion Sickness-Like Symptoms When Using Visual Devices. Hum. Factors 65:107–124. https://doi.org/10.1177/00187208211008687
- Schmäl, , 2013. Neuronal mechanisms and the treatment of motion sickness. Pharmacology 91, 229–241. https://doi.org/10.1159/000350185
- Reason, T., 1978. Motion sickness adaptation: a neural mismatch model. J. R. Soc. Med. 71, 819–829. https://doi.org/10.1177/014107687807101109
- Crowley, S., 1987. Simulator sickness: a problem for Army aviation. Aviat. Space Environ. Med. 58, 355–357.
- Dużmańska, , Strojny, P., Strojny, A., 2018. Can Simulator Sickness Be Avoided? A Review on Temporal Aspects of Simulator Sickness. Front. Psychol. 9, 2132. https://doi.org/10.3389/fpsyg.2018.02132
- IEEE Computer Society, IEEE Conference on Virtual Reality and 3D User Interfaces IEEE VR). https://www.computer.org/press-room/2020-news/ieee-vr-announces-all-virtual-venue-change-due-to-covid-19-concerns. (accessed 21 January 2022).
- Chessa, , Maiello, G., Borsari, A., Bex, P.J., 2019. The perceptual quality of the oculus rift for immersive virtual reality. Hum. Comput. Interact. 34, 51–82. https://doi.org/10.1080/07370024.2016.1243478
- Howarth, A., Costello, P.J., 1997. The occurrence of virtual simulation sickness symptoms when an HMD was used as a personal viewing system. Displays. 18, 107–116. https://doi.org/10.1016/S0141-9382(97)00011-5
- Kennedy, S., Drexler, J., Kennedy, R.C., 2010. Research in visually induced motion sickness. Appl. Ergon. 41, 494– 503. https://doi.org/10.1016/j.apergo.2009.11.006
- Sharples, , Cobb, S., Moody, A., Wilson, J.R., 2008. Virtual reality induced symptoms and effects (VRISE): Comparison of head mounted display (HMD), desktop and projection display systems. Displays. 29, 58–69. https://doi.org/10.1016/j.displa.2007.09.005
- McCauley, E., Sharkey, T.J., 1992. Cybersickness: perception of self-motion in virtual environments. Presence: Teleop. Vir. Environ. 1, 311–318. https://doi.org/10.1162/pres.1992.1.3.311
- Lin, J., Duh, H., Parker, D., Abi-Rached, H., Furness, T., 2022. Effects of field of view on presence, enjoyment, memory and simulator sickness in a virtual environment. Proceedings of IEEE Virtual Reality 164–17
- Kennedy, S., Stanney, K.M., Dunlap, W.P., 2000. Duration and exposure to virtual environments: sickness curves during and across sessions. Presence: Teleop. Vir. Environ. 9, 463–472 https://doi.org/10.1162/105474600566952
- Bashir, , Elsotohy, H.H., Elmoheen, A., 2020. Do Night Shifts Increase the Risk of Benign Paroxysmal Positional Vertigo Among Doctors and Nurses. J. Multidiscip. Healthc. 13, 963–966. https://doi.org/10.2147/JMDH.S256055
- Nagashima, , Osawa, M., Matsuyama, H., Ohoka, W., Ahn, A., Wakamura, T., 2018. Bright-light exposure during daytime sleeping affects nocturnal melatonin secretion after simulated night work. Chronobiol. Int. 35, 229–239. https://doi.org/10.1080/07420528.2017.1394321
- Hartstein, E., Behn, C.D., Akacem, L.D., Stack, N., Wright, K.P., LeBourgeois, M.K., 2022. High sensitivity of melatonin suppression response to evening light in preschool-aged children. J. Pineal. Res. 72, e12780. https://doi.org/10.1111/jpi.12780
- Neuhauser, K., von Brevern, M., Radtke, A., Lezius, F., Feldmann, M., Ziese, T., Lempert, T., 2005. Epidemiology of vestibular vertigo: a neurotologic survey of the general population. Neurology. 65, 898–904. https://doi.org/10.1212/01.wnl.0000175987.59991.3d
- Saredakis, , Szpak, A., Birckhead, B., Keage, H.A.D., Rizzo, A., Loetscher, T., 2020. Factors Associated With Virtual Reality Sickness in Head-Mounted Displays: A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 14, 96. https://doi.org/10.3389/fnhum.2020.00096
- Arns, L., Cerney, M.M., 2005. The relationship between age and incidence of cybersickness among immersive environment users, in: IEEE Proceedings. Virtual Reality, pp. 267–268. https://doi.org/10.1109/VR.2005.1492788
- Graybiel, , Wood, C.D., Miller, E.F., Cramer, D.B., 1968. Diagnostic criteria for grading the severity of acute motion sickness. Aerosp. Med. 39, 453–455.
- Kennedy, S., Lane, N.E., Berbaum, K.S., Lilienthal, M.G., 1993. A simulator sickness questionnaire (SSQ): A new method for quantifying simulator sickness, Int. J. Aviat. Psychol. 3, 203–220.
- Webb, A., Griffin, M.J., 2002. Optokinetic stimuli: motion sickness, visual acuity, and eye movements. Aviat. Space Environ. Med. 73, 351–358.
- Griffin, J., Newman, M.M., 2004. Visual field effects on motion sickness in cars. Aviat. Space Environ. Med. 75, 739–748.
- Gahlinger, M., 1999. Motion sickness. How to help your patients avoid travel travail. Postgrad. Med. 106, 177–184. https://doi.org/10.3810/pgm.1999.10.1.719
- Sherman, R., 2002. Motion sickness: review of causes and preventive strategies. J. Travel Med. 9, 251–256. https://doi.org/10.2310/7060.2002.24145
- Munafo, , Diedrick, M., Stoffregen, T.A., 2017. The virtual reality head-mounted display Oculus Rift induces motion sickness and is sexist in its effects. Exp. Brain Res. 235, 889–901. https://doi.org/10.1007/s00221-016-4846-7
- Tyrrell, , Sarig-Bahat, H., Williams, K., Williams, G., Treleaven, J., 2017. Simulator sickness in patients with neck pain and vestibular pathology during virtual reality tasks. Virtual Real. 22, 211–219. https://doi.org/10.1007/s10055-017-0324-1
- Zhang, L., Wang, J.Q., Qi, R.R., Pan, L.L., Li, M., Cai, Y.L., 2016. Motion Sickness: Current Knowledge and Recent Advance. CNS. Neurosci. Ther. 22, 15–24. https://doi.org/10.1111/cns.12468
- Altena, E., Daviaux, Y., Sanz-Arigita, E., Bonhomme, E., de Sevin, É., Micoulaud-Franchi, J.A., Bioulac, S., Philip, P., 2019. How sleep problems contribute to simulator sickness: Preliminary results from a realistic driving scenario. J. Sleep. Res. 28, e12677. https://doi.org/10.1111/jsr.12677
- Okada, , 2020. Nobel Prize Winners in Physiology and Medicine Gave Video Messages to “Japan XR Science Forum 2020 in US Midwest,” the International Science Forum a Variety of Researchers Joined With Their Families. https://www.businesswire.com/news/home/20200810005017/en/Nobel-Prize-Winners-in-Physiology-and-Medicine-Gave-Video-Messages-to-“Japan-XR-Science-Forum-2020-in-US-Midwest”-the-International-Science-Forum-a-Variety-of-Researchers-Joined-With-Their-Families (accessed 21 January 2022).
- UJA and Cheiron Initiative, UJA and Cheiron Initiative host world’s first virtual reality conference for researchers and their families “Japan XR Science Forum 2020 in the US Midwest.”
Supplements:
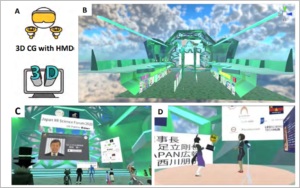
Supplemental Figure 1: Opening and award-giving ceremony at the main venue in a three- dimensional (3D)/head-mounted display (HMD) setting at Japan XR Science Forum 2020
- Platform that uses 3D computer graphics with an HMD
- Bird’s eye view of the venue, including the main venue and poster room.
- Participants represented by avatars. took part in the opening remarks from Kenichi Okada (Consulate-General of Japan in Chicago, IL, USA) in 3D space.
- Interactive trophy presentation with avatars that took place in the VR Chat format.
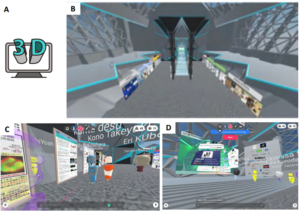
Supplemental Fig. 2: Poster tours and sessions at Hubs in a three-dimensional (3D) setting at the Japan XR Science Forum 2020
- Platform utilized 3D computer graphics.
- Overhead view of Mozilla Hubs.
- Poster-guided sessions, where the participants joined the scientific flash talk and question and answer sessions with social communication.
- Mirroring the main ceremony in the VR Chat in the Hubs room, which allowed all the participants to attend the session without a head-mounted display.
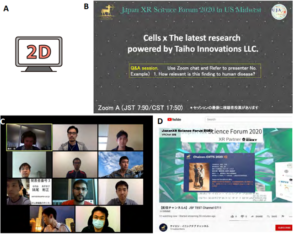
Supplemental Figure 3: Zoom and YouTube streaming in a two-dimensional setting at the Japan XR Science Forum 2020
- Platform utilized Zoom and YouTube.
- Workshop “Cell X the Latest Research Webinar” where participants could only view the presentation but could join the question and answer sessions using the chat function.
- Speakers and organizers joined the Zoom webinar with video cameras on.
- YouTube streams enabled the display of the main venue for all the participants without a head-mounted display or Zoom.
Supplemental Table 1: Questionnaire and answer options
| (7) Are there any recent changes in your physical condition that apply to you? (Please choose all that apply) | (1) None of the following (2) I have trouble sleeping (3) I am tired (4) I am stressed (5) I am pregnant (6) Others |
| (8) Have you ever experienced sick dizziness? | (1) Yes (2) No |
| (9) Do you get motion sickness easily? | (1) Yes (2) No |
| (10) If you are prone to motion sickness, what type of vehicle applies to you? (Please choose all that apply). | (1) Private cars (2) Trains (3) Buses (4) Airplanes (5) Ships (6) Swings and other playground equipment (7) Others |
| (11) Did you experience any dizziness or unusual sensations while attending this conference? | (1) Yes (2) No |
| (12) Did the symptom appear during your participation in the conference? | (1) Yes, it appeared during the conference (2) No, it appeared before the conference |
| (13) For those who had symptoms that appeared while attending the conference in the previous question, when did the symptoms start to appear after attending the conference? | (1) 0–0.5 hours (2) 0.5 –1 hour (3)1–2 hours (4)2–3 hours (5)3–4 hours (6)4–5 hours (7)5 hours or more |
(14) During which specific program did the symptoms appear?
(1) 7:00am Opening ceremony
(2) 7:50am Cells x the latest Research [Live]
(3) 9:20am Interdisciplinary exchange x Carrier
after studying abroad [Live]
(4) 10:50am Poster tours and session [Live]
(5) 11:20am Closing ceremony
Supplemental Table 2: Number of cybersickness onset in conference time schedule
| Elapsed time | Cybersickness (n) | |
| 0–0.5 hour | 4 | |
| 0.5–1 hour | 1 | |
| 1–2 hours | 2 | |
| 2–3 hours | 1 | |
| 3–4 hours | 0 | |
| 4–5 hours | 0 | |
| 5 hours or more | 0 | |
| Total | 8 |