Publication Information
ISSN 2691-8803
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2019
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Cure-Like Brain-Repair in a Girl with Atrophied Cerebellum and Pons through Coordination Dynamics Therapy
Giselher Schalow*
(NGOMR: Non-Government-Organized-Medical-Research), Switzerland
Received Date: March 30, 2021; Accepted Date: April 05, 2021; Published Date: April 16, 2021
*Corresponding author: Giselher Schalow, (NGOMR: Non-Government-Organized-Medical-Research), Dr. med. habil, Dr. rer. nat., Dipl. Ing. Untere Kirchmatte 6, CH-6207 Nottwil, Switzerland. Email: g_schalow@hotmail.com
Citation: Schalow G (2021) Cure-like brain-repair in a girl with atrophied cerebellum and pons through Coordination Dynamics Therapy. Adv Pub Health Com Trop Med 123: 1-47.
DOI: 10.37722/APHCTM.2021201
Summary
The cerebral palsy girl Sophie had from birth an atrophy of the cerebellum and ponds. At an age of 5.5, Coordination Dynamics Therapy was started. At the beginning, Sophie was incontinent and her speech was very poor. She could not stand, walk, run or jump. When falling, her protection automatism patterns were not working. The first fundamental progress in repair was achieved when the protection automatisms appeared in Sophie at an age of 6.5 years. The parents were not so much afraid anymore when trying to make her walking and Sophie tried now to walk by herself. The protection automatisms became operational at a time when she became able to exercise by herself on a special coordination dynamics therapy device. When the protection automatism occurred, the learning to walk became much easier and less risky. Sophie was not afraid anymore to fall and she tried herself now to walk without falling and she liked it. At an age of 8 she was able to walk without falling. Sophie’s trot gait crawling improved. The pace gait crawling became possible with poor performance. At an age of 9, Sophie could creep, crawl, upright, walk, jump and play with a ball. She was fully continent. Her speech had improved, so that the Author started to understand her. Her writing got better and her higher mental functions improved. She still had some problems with the balance, but she managed without falling. She was not able to run. The mother, teacher by herself, taught her at home. Through 6 years of CDT, at an age of 12 years, Sophie could fully manage the balance. She became able to run and jump freely and walk to a 1km distant supermarket for shopping.
Sophies cerebellar and pons repair is compared with the repair of a traumatic cerebellar and pons injury and her repair-stimulated development is compared with the development of healthy children in the age range between 3 and 18 years, quantified by coordination dynamics values and the ontogenetic landscape for locomotion, based on the System Theory of Pattern formation. Sophie could not fully catch-up so far with the normal development. Further therapy is needed. The health of normal pupils could be enhanced if the training on the special coordination dynamics therapy device would be included in school sport.
Keywords: Cerebellum Repair; Coordination Dynamics Therapy; Electrophysiology; Human Repair-Neurophysiology; Ontogenetic Landscape for Locomotion; Oscillatory Firing; Phase and Frequency Coordination; Single-Nerve Fiber Action Potentials; Surface EMG
Introduction
It has been shown that Coordination Dynamics Therapy (CDT) can improve or repair central nervous system (CNS) functioning after stroke [1], traumatic brain injury [2, 3], spinal cord injury (SCI) [4-8], cerebellar injury [9], cerebral palsy [10], hypoxic brain injury [11], in Parkinson’s disease [12], spina bifida (myelomeningocele) [13] and scoliosis [14]. Speech had been induced and improved in a patient with severe cerebral palsy [15]. A permanent coma patient could be brought out-of-coma and relearned to speak [16]. Cancer grows could be inhibited through CDT [17, 18]. Cardio-vascular performance could be improved. There is indication that the general health can be improved via CDT to live longer with a better quality of life for 10 to 20 years.
I this case report, it will be shown that, based on human repair-neurophysiology, the cerebral palsy girl Sophie with an atrophied cerebellum and pons could nearly be cured from her malformation through the movement-based learning therapy called CDT. Such great repair of a malformation became possible through on an efficient human science-based CNS repair method, administered aggressively with up to 20 hours therapy per week for 6 years.
This powerful repair in cerebral palsy indicates that disabilities are diseases, which can partly be cured through movement-based learning, especially in children under 10 years of age. The problem with such learning therapy is that there is a lot of mental discipline necessary for the family and the patient. No real help is coming from the mainstream medicine. With respect to the repair of the CNS, mainstream medicine is something like 30 years out-of-date. Too much research and health insurance money is wasted in inefficient treatments. Human repair-neurophysiology is not organized and real expert knowledge is not of interest to the society. Medical faculties of universities are not trying to get up to date for teaching and medical research. Movement-based learning is besides drug therapy and operations a third leg of medicine. Since the nervous system is involved in nearly all body functions, an improvement of nervous system functioning will improve the health in general.
In the Method, the human-science-based CDT is shortly introduced and applied to the repair of the CNS, including the cerebellum and pons. It will be shown that Sophie got a senseful life through human neuroscience. In the Results, the improvement of CNS functioning through CDT is displayed step by step. In the Discussion, the repair of the atrophy of cerebellum, pons, and may be some other malformed CNS structures, is compared with the repair of a traumatic cerebellum and cerebrum injury. The repair-induced development of Sophie is compared with the development of the healthy brother and healthy girls and boys, quantified by the low-load coordination dynamics values.
Method
Human Neurophysiology
With the single-nerve fiber action potential recording method, single-nerve fiber action potentials can be recorded from sacral nerve roots, running in and out of the spinal cord (Figure 1) [19].
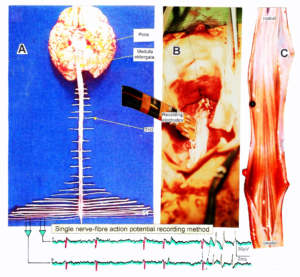
Figure 1: Layout of the recording of single-nerve fiber action potentials to analyze the self-organization of neuronal networks of the human CNS under physiologic and pathophysiologic conditions. A, B, C. By recording with two pairs of platinum wire electrodes (B) from sacral nerve roots (cauda equina, C) containing between 200 and 500 myelinated nerve fibers, records were obtained in which single nerve-fiber action potentials (APs) were identified from motoneurons (main AP phase downwards) and afferents (main AP phase upwards). A. Human CNS with the schematic illustration of the recording layout and an original record of single nerve-fiber action potentials. Note the time calibration of 2ms. B. Intraoperative recording layout (when implanting a bladder stimulator) with two pairs of wire electrodes and one temperature sensor. A thin nerve root is positioned over the platinum wire electrodes. C. Dissection of the human cauda equina. At the caudal end, the filum terminalia and thin nerve roots can be seen. Dissections of the Author apart from the laminectomy in B.
By measuring the conduction times and with the known electrode pair distance of 10 mm, conduction velocity distribution histograms were constructed in which the myelinated nerve fiber groups larger than 4mm could be characterized by group conduction velocity values (Figure 2). After the recording, morphometry was performed. Distributions of nerve fiber diameters were constructed and nerve fiber groups were characterized by the peak values of asymmetrical distributions (Figure 2). By correlating the peak values of the conduction velocity distributions with those of the diameter distributions, obtained for the same root, a classification scheme was constructed of the human peripheral nervous system (Figure 3) [20, 21]; the only existing one for human peripheral nerve fibers.

Figure 2: Development of a classification scheme for human peripheral nerve fibers. Conduction velocities (V) and nerve fiber diameters (Æ) of afferent (from receptors) and efferent (motor) nerve fiber groups in normal humans and in patients with a traumatic SCI for 0.5 to 6 years.
This classification and identification scheme represents a solid basis for classifying and identifying nerve fiber groups in the human Peripheral Nervous System (PNS) and analyzing Central Nervous System (CNS) functions at the single-neuron level. It became thus possible to record natural impulse patterns simultaneously from identified single afferent and efferent nerve fibers and to analyze self-organizing mechanisms of the human CNS under physiologic and pathologic conditions.

Figure 3: Classification scheme for human peripheral nerve fibers. Conduction velocities (V) and nerve fiber diameters (Æ) of afferent and efferent nerve fiber groups in normal humans and in patients with a traumatic spinal cord injury for 0.5 to 6 years. The splitting of the a1-motoneurons into the 3 subgroups, a11, a12, a13, has not yet been confirmed. This is the only existing classification scheme for human peripheral nerve fibers!
The most important finding with the single-nerve fiber action potential recording method was that nerve cells in the human CNS are organizing themselves through “Phase and Frequency coordination”[22, 40] (Figures 6, 50). In nerve fibers, this phase and frequency coordination can easily be measured, because the three motoneuron types fire for high activation oscillatory [23] and offer in this way a structure to which the timed firing of neurons can be related to. Since the α2-motoneuron oscillations are most stable, firing phases of neurons can be related best to the α2-motoneuron firings.
Figure 4 shows schematically the oscillatory firing patterns of the three kinds of motoneurons and the muscle fiber types they innervate.
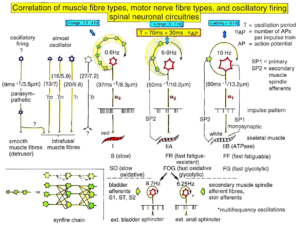
Figure 4: Correlation of muscle fiber types, motor nerve fiber types, and oscillatory firing spinal neuronal networks (oscillators), based on histochemical, morphological and neurophysiological properties. This figure provides a simplified correlation between muscle fiber, motoneuron and sacral oscillator types. No additional subtypes have been included. The existence of a1-motoneuron (FF) oscillators firing at 10 Hz has been predicted and they have been identified in paraplegics. a = motoneuron, g1, g2 = dynamic and static fusimotors, parasympathetic = parasympathetic preganglionic motoneuron. S1, ST, S2 = stretch, tension and flow receptor afferents.
By comparing CNS functioning in brain-dead humans (where the spinal cord is functioning rather physiologically) and patients with spinal cord injury, injury-induced changes of CNS functioning can be measured and partly repaired. Mainly the phase and frequency coordination of neuron firing becomes impaired following injury. This impaired coordination among neuron firings can efficiently be repaired through exercising on the special CDT device (Figures 19-21).
The drawing back of the single-nerve fiber action potential recording method is that it is an invasive recording method. But with the surface electromyography (sEMG) [24] one can record non-invasively coordinated firing among motoneurons via their motor units if one records from suitable patients, like incomplete spinal cord injury patients, when a certain muscle is only innervated by a few motoneurons.
In Figure 5, the recordings from motoneurons and motor units are compared. The firing patterns of α1, α2 and α3-motoneurons can easily recorded with the single-nerve fiber action potential recording method but not with the sEMG (Figure 5). From spinal cord injury patients, on the other hand, single-motor unit APs can be easily recorded from α1 motor units but not from α2 and α3 motor units (Figure 5), because their AP amplitude seems to be too small. Clinical sEMG recordings therefore show mainly the activity of α1 motor units. The generation of motor patterns of α1-motoneuron firings with increasing load and the phase and frequency coordination among single-motor unit firings can be recorded with sEMG (Figure 6).

Figure 5: Oscillatory firing patterns of a1, a2, and a3-motoneurons recorded from motoneuron axons with the single-nerve fiber action potential recording method and by surface electromyography (sEMG) from FF, FR, and S-type motor units. The left panel shows original recordings, the middle panel the schematic patterns; the recording methods are indicated on the right side. The recordings were taken from patients with spinal cord injury and Parkinson’s disease and from brain-dead humans.
The neural networks of the human brain, including the cerebellum, organize themselves by phase and frequency coordination among neuron firings and neural sub networks as for example the network oscillators of which the motoneuron is a part.This coordination is achieved by the organization tendencies of the network, the descending impulse patterns from the brain and the spatiotemporal afferent impulse patterns from the periphery.
If the premotor spinal oscillators would not coordinate their firing and synchronize their firing for longer periods of time, tremor would occur. Such pathologic synchronization can be observed in patients with Parkinson’s disease [25, 40]. If the neural networks are damaged by trauma, degeneration or malformation, the coordination between neuron firings becomes impaired and has to be repaired by movement-based learning (CDT). Drugs and operations cannot repair neural network functioning.

Figure 6: Phase and frequency coordination between oscillatory firing of 3 motor units (FF-type, motor units ‘2’ and ‘3’ are partly marked) during the generation of a motor program when exercising on the special coordination dynamics therapy device at loads increasing from 100 to 200N. Oscillation periods (T) and oscillation frequencies (f [Hz]) of oscillatory firing motor unit 1 (largest motor unit) are partly indicated. ‘C, F’ soleus electrodes shifted to gluteus muscles. In ‘F’, some coordination’s between motor unit ‘3’ and ‘1’ are marked.
Improvement of the Stability and Exactness of Phase and Frequency Coordination to Allow Specific Patterns Formation and Learning Transfer (System Theory of Pattern Formation)
The importance of stable and exact phase and frequency coordination, to allow specific pattern formation and in consequence learning transfer [26] to other patterns, can be understood at the collective variable level (System Theory of Pattern formation [27-29]) and at the neuron level. The behavioural information Finf of the coordination pattern dynamics, characterized by equations of motion of collective variables, dX/dt = Fintr(X) + ∑cinfFinf(X,t), affect the whole coordination pattern dynamics, including stability, rather than only certain coordination patterns. If the behavioural information includes the exercising of extremely coordinated, integrative movements, like exercising on the special CDT device for turning, then the quality of CNS self-organization can be enhanced by improving the exactness of self-organization, namely the precision of phase and frequency coordination between neuron and neural assembly firings. By improving the precision of organization of the intrinsic dynamics Fintr(X), that is, the specific variability of the injured networks, certain patterns do then already reappear. In the patient Sophie, the protection automatisms appeared with the improvement of CNS functioning, first time in her life.
Neurons often serve more than one network pattern at the same time by time sharing of neuron firing and, in this way, give rise to learning transfer among the activated patterns. If sub networks are improved in the organization of one pattern, the organization of the other pattern will also improve. Neurons involved in the organization of breathing and activating intercostal muscles, for example, are also involved in the organization of trunk stability. By reducing the spasticity of the trunk (in patients with Parkinson’s disease), the breathing will also improve. Similarly, sphincteric motoneurons are involved in continence and pelvic floor weight bearing. If during pregnancy the pelvic floor is not trained, sometimes incontinence occurs. This stress incontinence after birth can be repaired by learning transfer from coordinated movements. By mainly exercising on the special CDT device and jumping on springboard, urinary bladder functions can be repaired by learning transfer in healthy women. Also the girl Sophie became continent in this way.
Measuring CNS Functioning by the Arrhythmicity of Exercising (Coordination Dynamics Value)
The impaired phase and frequency coordination at the single neuron level, the assembly level and the macroscopic level can be measured macroscopically when the patient is exercising on a special coordination dynamic therapy device (Figures 19-21) on which arms and legs turn with a slightly different frequency (transmission 19 (arms) : 18 (legs)). The phase coordination between arms and legs is imposed by the device. The loss of phase and frequency coordination between arm and leg movements becomes visible and measurable by the arrhythmicity of turning. During a turning cycle the coordination between arms and legs changes between pace and trot gait and according to the difficulty of the coordination, the turning frequency increases and decreases. This frequency variation (df/dt; f = frequency) can be recorded, quantified and displayed on a computer screen (Figure 27) and is called coordination dynamics value. CNS functioning is therefore measured though pattern change (continuous change from trot gait to pace gait) according to the System Theory of Pattern Formation.
During the functional reorganization of the injured CNS of patients, the relative phase and frequency coordination of neuron firing has to be entrained as exactly as possible by the movement induced afferent impulse patterns from the receptors (learning through feedback information) to restore coordination in the range between 3 and 5 milliseconds (approximate lengths of postsynaptic potentials). The device has therefore to impose the exercising patient a coordination in the millisecond range for the different coordination’s of arm and leg movements between pace gait and trot gait. The easy pace and trot gait coordination’s, but not the difficult intermediate coordination’s, can often be performed by the patient easily. Therefore, the continuous change from the easy to the difficult coordination’s and backwards diagnoses the capability of the CNS to organize easy and difficult organizational states. If the movement states can be easily generated by the neuronal networks of the CNS, then the frequency variation of turning is small during the turning cycle, and if the movement state is difficult to be organized by the CNS, then the frequency variation is large (the coordination dynamics value is large).
Unique Properties of Special CDT Devices
The special CDT device has three important properties. First, the patient performs coordinated arm, leg and trunk movements when exercising on it. The training of integrative patterns take care of that the pathologic organization cannot escape from repair by shifting to another part of the CNS and the whole CNS, including the injured parts, is reorganized so that other CNS parts can take function over through plasticity. Second, the device is extremely exact, so that the endplate potentials in the neural networks (approximately 5ms long) overlap, to improve the efficiency of organization. In spinal cord injury, for example, the transmission over the injury site will increase. Third, the coordination between arm and leg movements changes from pace to trot gait, imposed by the device. The intermediate coordination patterns between pace and trot gait are difficult to generate for the CNS neural networks. If the patients CNS learns to generate these intermediate patterns, imposed by the device, then the neural networks have learned to function better in the deep complexity of CNS organization. The patient’s nervous system learns by turning from the device, to function more physiologic through improving especially the phase and frequency coordination among neuron firings. This phase and frequency coordination can be measured by the single-nerve fiber action potential recording method (Figure 50) invasively and by single-motor unit surface electromyography non-invasively (Figure 6).
Motor Learning and Problem-Solving Therapy
Because of atrophied cerebellum and pons in a patient, there is retarded, accelerated or deviant development of motor and other functions. Some functions may not develop at all, while others show only a decrease in variability. Both impaired and healthy parts of the brain mature over time and thus lead to increased complexity, which has direct repercussions on the quality of the learning (trial-and-error-elimination [30]) processes. Processes that in themselves are normal cannot bring about good results because some areas of the brain which are also necessary for the accomplishment of the particular motor function are deficient.
The well-known symptoms and signs of cerebral palsy in the first year of life (poverty of movements, stereotypy of posture and motility, inability to “discover” new motor possibilities, neglect of one extremity, stereotyped extension of the legs during vertical suspension, head-lag during the traction test or during sitting) can all be traced back to a lack of trial-and-error-elimination processes (learning) as a consequence of deficient brain structure. In the case of an inability to “discover” new motor possibilities, there may be a disturbance in the chain of events because errors are not recognized (or not eliminated), with the result that the processes stop prematurely [31]; the learning therapy has therefore to be administered continuously over longer times to run through the whole chain of events.
The System Theory of Pattern Formation of CNS development encompasses all areas of development and is derived from mathematics, physics, human neurophysiology, clinical research, and developmental psychology. The CNS is considered as one neuronal network. A new behavior is generated, which is dependent on the input of all subsystems. This behavior may have a characteristic that could not have been determined by evaluating the contributing behaviors individually [32].
The system repair approachis a “feed-forward system” that is self-correcting ‘en route’ rather than hardwired from the cerebral cortex. It also implies that all factors, subsystems, or structures contributing to the motor behavior (or patterns in general) are important and exert an influence on the outcome [32]. If the cerebellum and pons are atrophied in an infant, then many patterns become abnormal or do not exist. The higher centers can no longer control movements or other patterns sufficiently. But through movement-based learning, a self-correction ‘en route’ may partly compensate for the missing contribution of a subsystem in the way that other subsystems take functions over and/or the cerebellum and pons are partly repaired.
The problem-solving learning tries to repair sub-networks that are necessary for functioning and learning. By inducing trial–and-error-elimination processes in subunits of the normal developing nervous system, an optimal development is achieved [30]. To teach the injured CNS to repair itself by trial–and-error-elimination processes, the CNS has to recognize upon CDT which sub-networks, regulation units or sub loops are not functioning properly (or are missing) and to repair them by error elimination, including the possibility that other brain parts partly take functions over, and sub-networks build anew to a limited extent.
Functional Anatomy Pons and Cerebellum
The patient Sophie had the diagnosis of cerebral palsy with ataxia and speech developmental retardation. Because of a prolonged postnatal icterus, the basal ganglia may have been damaged. At an age of 4.5 years an MRI was performed to update the diagnosis. A severe cerebellar atrophy with accompanied atrophy of the ponds was found. Especially the cerebellar hemispheres and the vermis were atrophied. No pathology of the basal ganglia, no myelin sheath disturbance and no signs of postnatal ischemia were found. The CNS repair strategy of Sophie was therefore to concentrate on the repair of the cerebellar and pons atrophy, even though other mild atrophies/injuries of other brain parts cannot be excluded.
The cerebellum (Figure 7) is the central organ for fine motor control and modulates the activity of motor nuclear areas in the brain and spinal cord. Cerebellar injuries manifest themselves clinically with disturbance of movement, balance, speech and urinary bladder functioning.
Functionally and phylogenetically, the cerebellum is anatomically divided into three components: the vestibulocerebellum (flocculonodular lobe), the spinocerebellum (vermis and paravermian zone, it receives most of its afferent input from the spinal cord) and the cerebrocerebellum (the two cerebellar hemispheres). The cerebrocerebellum (youngest portion of the cerebellum) occurred during phylogenetic development with the expansion of the cerebrum and the transition to an upright stance and gait. The two cerebellar hemispheres have an intimate functional connection to the cerebral cortex, which projects to it by way of the pontine nuclei (Figure 8).

Figure 7: Cerebellum. Above left side: division into vermis, pars intermedialis, and pars lateralis. Right side: division into vermis, anterior lobe, and posterior lobe. The anterior and posterior lobes are separated by the primary fissure. (From Duus [34]).
Figure 8: Afferent and efferent connections of the cerebellum with other parts of the nervous system (from Duus [34]).
The cerebellum may not only be responsible for fine motor control but may also store important movement automatisms. It processes information from multiple sensory channels (particularly vestibular sense, touch, proprioception, bladder fullness sense, vision and hearing), together with motor impulses, and modulates the activity of motor nuclear areas in the brain and spinal cord. Cerebellar injuries (and atrophy) manifest themselves clinically with disturbances of movement, balance, bladder functioning and loss of protection automatisms. The cerebellum plays a major role in motor learning and memory. The disturbance of movement and balance includes the disturbance of cerebellar regulatory circuits which have to be repaired.
Important regulatory circuits do exist. A long regulatory loop is created, travelling from the cerebral cortex to the pontine nuclei, cerebellar cortex, dentate nucleus, thalamus, and finally back to the cortex (Figure 9A, D). The cerebellum gets an efference copy of motor activity for processing. A further regulatory circuit comprises the triangle of Guillain and Mollaret, travelling from the red nucleus by way of the central tegmental tract to the olive, then to the cerebellum and back to the red nucleus (Figure 9B). The cerebellum influences spinal motor function by many descending tracts (Figure 10) including the rubrospinal and the reticulospinal tract (Figure 9C).
The repair of the impaired phase and frequency coordination of neuron firing (Figure 6) in the neural networks, when exercising on a special CDT device (Figure 9D), means that also the coordinated firing of neurons in the regulatory circuits has to be repaired. Otherwise, the regulatory circuits cannot sufficiently regulate movement and other functions. Furthermore, the organization in the nuclei has also to be repaired with respect to the coordinated firing of their neurons. As will be shown below in the patient Sophie, the improvement of phase and frequency coordination of neuron firing had tremendous consequences for the improvement of her movements.
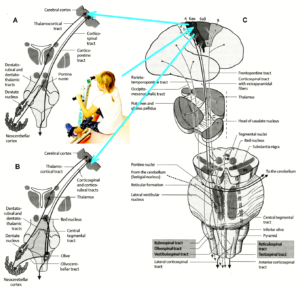
Figure 9: Cerebellar regulatory circuits involving the pontine nuclei (A) and the olive (B, triangle of Guillain and Mollaret). The cerebellum influences spinal motor functions by way of fibers traveling from the red nucleus, reticular formation, olive, tegmental nuclei and vestibulocerebellum (C). A damage or atrophy of the cerebellum and ponds must have tremendous consequences for balance and walking performance. (From Duus [34]).

Figure 9D: The cerebral palsy girl Sophie during exercising on a special CDT device. At the same time, the mother (teacher herself) is administering speech therapy to her. If Sophie would stop turning, because she has problems to perform two patterns at the same time, the mother could support the turning movement of Sophie with one hand (not doing in this moment). In such very integrative training setting, nearly the whole somatosensory and motor cortical fields are activatedwith their associated fields. Of course, the important cerebellar regulatory circuits (Figure 9A, B) get also the integrative coordinated input for regulation.Such combination of movement and speech therapy is therefore very efficient for repair. Becausethe hand leavers pass through the field of vision of Sophie, speech, movement and vision are activated in coordination. – Cortical fields are taken from Penfield W and Rasmussen T, New York, 1950). – This special CDT device for measuring and therapy (int.pat.) is produced by the firm: Giger Engineering, Martin Giger dipl.Ing.ETH/SIA, Herrenweg 1, 4500 Solothurn, Switzerland, www.g-medicals.ch.
The vestibulocerebellum, the spinocerebellum and the cerebrocerebellum have different functions in the coordination of movement which become apparent in cerebellar injuries. It seems that if the cerebellar cortex is injured, other portions of the brain can assume some of the functions. If the deep cerebellar nuclei are impaired minimal recovery is likely to occur.
The vestibulocerebellum receives impulses from the vestibular apparatus carrying information about the position and movements of the head. Its efferent output influences the motor function of the eyes and body in such a way that equilibrium can be maintained in all positions and with any movement.
The spinocerebellum controls muscle tone and coordinates the actions of antagonistic muscle groups that participate in stance and gait. Its efferent output affects the activity of the anti-gravity muscles and controls the strength of forces induced by movement (e.g., inertia and centrifugal force).
Injuries of the anterior lobe and of the superior portion of the vermis in and near the midline produce ataxia of stance and gait. The gait ataxia (abasia) produced by such injuries is worse than the ataxia of stance (astasia). During the process of repair by learning, Sophie with an atrophy of the vermis, had more problems to learn to walk and run than to stand freely.
The cerebrocerebellum receives most of its neural input indirectly from extensive portions of the cerebral cortex, mainly Brodmann areas 4 and 6 (the motor and premotor cortex) via the corticopontine tract (Figure 9A, C) but also, to a lesser extent, from the olivocerebellar tract (Figure 9B). The cerebellum receives advance notice of any planned voluntary movement initiated in the cerebral cortex, so that it can immediately send modulating and corrective impulses to the motor cortex through the dentatothalamocortical pathway (Figures 8, 9A). The dentate nucleus also projects to the parvocellular portion of the red nucleus. This dentate-rubro-olivo-cerebellar feedback loop (Figure 9A) plays an important role in neocerebellar impulse processing.
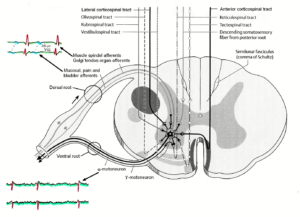
Figure 10: Synapses of the descending motor tracts onto anterior horn motoneurons. The motoneuron is a summing point. It is getting many inputs including those from the periphery (reflexes) and from many descending tracts. The simultaneous input from the reticulospinal tract could give rise to α- and γ-motoneuron co-activation. In difference to the picture, dorsal and ventral nerve roots fuse before the ganglion (see Figure 1A).
The complex connections of the cerebellum enable it to regulate all directed movements smoothly and precisely. By way of the very rapidly conducting afferent spinocerebellar pathways (Figure 11), it continuously receives real-time information about the activity in the periphery. It can thus take action to correct any errors in the course of voluntary movement to ensure that they are executed smoothly and accurately.
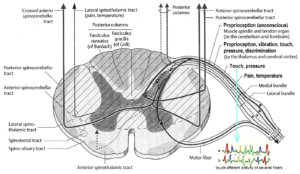
Figure 11: Anterior and posterior spinocerebellar tracts (from Duus [34]). Single-nerve fiber activity of several touch fibers (conduction velocity ≈ 44m/s (Figure 3)) are indicated, which may contribute to the spinocerebellar tracts because the conduction velocity is high. Primary spindle afferents (and a1-motoneurons) conduct at a velocity of 60m/s (Figure 3)).
It was argued above that the phase and frequency coordination among neuron firing in the neural networks is efficiently improved when exercising on the special CDT device. More precisely with respect to cerebellum injury, the phase and frequency coordination between neuron firing is improved in regulation units like in Figures 9A, B and in the organization patterns in the nuclei as for example in the dentate nucleus. The cerebellum obtains an efference copy of the performed movements via the pontine nuclei (Figure 9A) and receives at the same time real time information about the motor activity in the periphery (muscles, tendons, joints; spinocerebellar tracts (Figure 11)). Volitional movements and automatic movements can thus be performed smoothly and precisely.
With injury or atrophy of the cerebellum, the movements cannot any more performed smoothly and accurately. The impairment depends on the actual injuries of the cerebellum and pons nuclei/tracts.
Automatisms are absolute necessary for everyday life and make life easier. The automatisms creeping, crawling, up-righting, walking and running are used in CDT for nervous system repair. It is believed that inborn automatisms and learned automatisms are stored in the cerebellum and can be recalled from it at any time precisely, rapidly and relatively effortless. In cerebellum injury these inborn and learned automatisms are impaired or lost. In difference to the computer, the automatisms can be repaired by learning. In the language of computer, the automatisms can be re-learned by improving software and hardware as will be shown in the cerebral palsy girl Sophie.
Some theory of Coordination Dynamics Therapy, including original recordings of single-nerve fiber action potentials from human, and treatment of the patient Sophie can be followed up on a video film with the heading ‘From brain repair to Covid-19 treatment via Coordination Dynamics Therapy’ [33]. Actually, the new method of recording single-nerve fiber action potentials from human peripheral nerve fibers was the main step to develop Coordination Dynamics Therapy for repairing the human CNS.
Repair Strategies at the Neuron Membrane and Genetic Level
The building of functions/patterns in the young cerebral palsy patient, first time in life, make it likely that excitation-neurogenesis coupling [35] contributed, stimulated through CDT.
- Repair depends on learning and memory formation, mediated or supported by epigenetic mechanisms. Epigenetics is the interplay between genes and the environment resulting in phenotype and epigenetic landscape.
- Epigenetic mechanisms, like DNA methylation, are probably sensors for movement-based learning and memory formation and fine modulators of neurogenesis though CDT (Figure 12).
- The epigenome consists of non-coding RNA and chromatin, a proteinaceous matrix surrounding DNA. The dynamic interactions of post-translationally modified chromatin proteins, covalently modified cytosines inside DNA and non-coding RNA define the complex pattern of gene expression beyond the four bases of DNA.
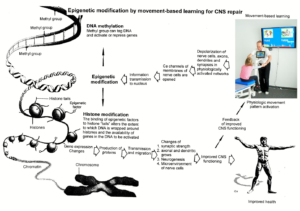
Figure 12: Epigenetic regulation for repair by movement-based learning. CDT-induced stimulation of the pathways that regulate neural network repair is a proven therapeutic and preventive tool. Epigenetic mechanisms, stimulated by physiologic network activation, are likely key players within signaling networks, as DNA methylation, chromatin remodeling and small non-coding RNAs superfamilies’ are required for the fine-tuning and coordination of gene expression during neural network repair by learning.
- The hippocampus plays an essential role in learning and memory. In the hippocampus there exists a specialized form of neural plasticity, which is, the generation of new functional neurons from stem cells occurring throughout life. Adult hippocampal neurogenesis contributes to learning and memory formation.
- New neurons are important for learning and memory formation (besides functional reorganization), i.e., for increasing the rate of repair, for the following reasons:
- The insertion of new neurons helps to store the memory of the same activity that led to the creation of the neuron.
- Activity-dependent neurogenesis enhances the learning of new memories and degradation and clearance of previously stored unwanted memories like spasticity, because the synapses, dendrites and axons can be devoted more fully to the newer memories. The old neurons with large and complex axon and dendritic trees are difficult to change. They can only be changed with sustained effort.
- New neurons seem to improve the accuracy of relearned patterns (from model study [35]). This means that new neurons help to improve phase and frequency coordination of neuron firing and pattern stability.
- The advantage of new neurons seems to be dramatically greater in networks that had been more active and had been required to store more memories [35]. The advantage of neurogenesis for memory storage in heavily active networks is that it provides an increased rate of repair if movement-based learning is administered aggressively and if different movements are trained.
- Specific natural network activity is required for multiple aspects of Specific activity is essential for correct migration of interneurons and it also controls the development and repair of their axons and dendrites. During repair there is a specific requirement of network activity in shaping the cortical integration of specific neural subtypes. Newly build neurons are likely electrically active shortly after their birth and participate in the early network activity that contribute to circuit maturation during repair by CDT.
- Specific activity is required for migration and maturation at several stages of repair. A break in CDT may invalidate the whole chain of repair events. Specific interneuron subtypes require activity for migration and morphological maturation at two distinct stages of development [35]. Newly built neurons may even require specific activity for migration and maturation at several distinct stages of repair. During a break in CDT, the specific activity, required for neuron migration, maturation and network integration may not be supplied at one of these stages so that the chain of repair events is severed and the whole repair chain has to be started anew.
- Drug application may undermine repair. Altering the level of neuronal excitability within genetically targeted neurons from drug application, for example antiepileptic drugs may have profound consequences on multiple aspects of the repair of select types of neurons within a population of neurons, as well as their associated gene expression. The pain-killer ‘Contergan’, taken during pregnancy, changed gene expression and the babies were born without arms.
- Excitation-neurogenesis coupling [35]:
- Excitation increases or decreases neuron production directly by excitation-neurogenesis coupling.
- The excitation acts indirectly on the surrounding mature (hippocampal) cells through depolarization-induced release of growth factors.
- Adult neurogenesis is enhanced by excitatory stimuli and involves Ca2+ channels and NMDA receptors.
- The Ca2+ influx pathways are located on the proliferating stem/progenitor cells (NPCs), allowing them to directly sense and process excitatory stimuli. The Ca2+ signal in NPCs leads to rapid induction of a proneural gene expression pattern.
- Integrative coordinated movements have to be trained to allow functional reorganization and new nerve cell integration across very large distances. CDT has to activate injured and uninjured networks to enhance physiologic CNS functioning and learning transfer.
- Conclusion for optimal therapy according to the present stage of knowledge. If there is similarity between development and repair, animal (mice) data also hold in humans and the principles of neurogenesis of the hippocampus also hold in other parts of the brain, albeit to a much lesser extent, then the patient has to be trained at his limits (1) to induce substantial building of new nerve cells [36]. The treatment has to be continuously administered (2) to support all stages of repair at the progenitor level as migration, maturation and integration. The networks requiring repair have to be activated specifically (3) to generate repair-friendly, micro-environmental properties in the networks. No drugs should be administered that change neuron excitability (4). The exercises have to include coordinated arm, leg and trunk movements (if possible) to improve the impaired phase and frequency coordination for CNS self-organization (5). The performed movements have to be as integrative as possible to reconnect distant brain parts and to induce learning transfer.
This very short introduction to the theory of coordination dynamics therapy may help to understand the substantial progress achieved in the cerebral palsy girl.
Results
Cerebellum repair within 12 months of CDT

Figure 13: The cerebral palsy Sophie when trying to walk with her mother before CDT was started. She could not generate a walking pattern. Knees were overstretching (A) which blocks the walking pattern and she was immediately falling (B).
At the beginning of CDT, the 5.5-year-old Sophie could not perform any movement accurately. She was incontinent and her speech was poor. The Author could not understand her. She could crawl on the floor in trot gait coordination with poor performance. Pace gait crawling was not possible.
Of course, Sophie could not walk. When the mother tried to walk with her, she was more hanging in her hand than walking (Figure 13). There was no real walking pattern and no balance. She could not really learn it, because she had no protection automatism when falling, which is probably normally stored in the cerebellum. If she would fall, she would injure herself, of what the parents were very afraid of.

Figure 14: The CP girl Sophie during jumping on a trampoline (A), during supported jumping on springboard with the mother (B) and during free jumping on springboard (C, D).
Sophie could not jump because she did not have that pattern learned and stored in her CNS and jumping is no automatism. She learned the jumping slowly and hated it. First, she could jump a little bit by herself on a trampoline (Figure 14A). The jumping on springboard was harder to learn. The supported jumping was a big load for the parents, because Sophie contributed only little (Figure 14B). Slowly she contributed more and more and at the end she could jump by herself on springboard, but with poor performance (Figure 14C). When she had learned the jumping, she liked it.

Figure 15: Improvement of CNS functioning of the CP girl Sophie, quantified by jumping on trampoline (A), jumping on springboard (B) and walking without falling (C).
The first improvement in movements is shown in Figure 15. She started the continuous jumping with one jump (Figure 15A, B) and the walking with two steps (Figure 15C). The progress of learning was slowly. With a second intensive training (Figure 15C), the learning process speeded up.
The first fundamental progress in repair was achieved when the protection automatisms appeared in Sophie at an age of 6.5 years (Figure 17A). The parents were not so much afraid anymore when trying to make her walking and Sophie tried now also by herself to walk. The protection automatisms became operational at a time when she became able to exercise by herself on the special CDT device (Figure 21). Also, the assessment of low-load CD values became possible (Figures 27, 28).
When she became able to perform the automatism creeping, some malformations of the cerebellum became visible. When Sophie crept in interpersonal coordination with the patient Nefeli (SCI), and she liked it very much to copy Nefeli’s movements, her inaccurate performance became apparent (Figure 16). Nefeli crept physiologically, apart from the wrong positioning of the right foot and the dorsal flexion of the pelvis due to trunk spasticity. Since Nefeli and Sophie were creeping, balance was not needed and the vestibulocerebellum was not or only little activated.
Figure 16 shows, in comparison to the performance of Nefeli, that Sophie’s legs were moving uncoordinated about (Figure 16K) even though Sophie was crawling in interpersonal coordination with Nefeli. The leg functions were more impaired than the arm functions. She could also better stand (Figure 16L) than walk (see below). This indicates an injury of the anterior lobe and the superior portion of the vermis in and near the midline of the spinocerebellum [34]. Such injury produces ataxia of stance and gait and the gait ataxia (abasia) is worse than the ataxia of stance (astasia). A broad-based, unsteady gait was not observed in Sophie (Figures17H, 18C) with her cerebellum atrophy, but was observed in an adult patient with a severe traumatic cerebellum injury (Figure 18D).

Figure 16: Creeping in interpersonal coordination of the CP girl Sophie with an atrophy of the cerebellum and pons with the patient Nefeli, who had suffered an incomplete SCI at the level of Th10. Note the partly uncoordinated leg movements of Sophie in spite of no balance problems. Nefeli was crawling rather physiologically. When Nefeli was lying relaxed on the floor, trunk spasticity did not occur (M) and pulling the pelvis dorsally.
From Figure 16B it can be seen that Sophie was overstretching the left leg during creeping. The inability to stop the leg movement on time is called dysmetria (past-pointing, overshoot; hypermetria [34]). For sure Sophie had also dyssynergia; the loss of the precise cooperation of multiple muscle groups in the execution of a particular movement (creeping). Each muscle group contracts, but the individual groups fail to work together correctly. This severe impairment of the execution of voluntary movement is due to the atrophy of her cerebrocerebellum (Figure 7).
The learning to walk was extremely difficult. The parents tried hard to have Sophie not in the wheelchair for the rest of her life. When the protection automatism occurred (Figure 17A), the learning of walking became much easier and less risky. Sophie was not afraid to fall and tried herself to walk without falling and she liked the walking. Figure 17 shows how Sophie was getting up (Figure 17B-G) after falling (Figure 17A). Interesting is that Sophie started to walk (Figure 17F) before she was fully in the upright position (Figure 17G). She was able to combine the movement ‘getting up’ and ‘walking’. This indicates that certain functions in her cerebellum were working physiologically. At the beginning, the rather physiologic walking pattern as in Figure 17H, with a too large stride length, was achieved only sometimes. The stability of the walking pattern was low and also the stability of the balance was low. Probably there was also some atrophy in the vestibulocerebellum. Her nervous system had to achieve three goals: First to have a higher stability of the walking pattern, second to improve the stability of the balance pattern and third to combine both patterns. The fundamental hope for Sophie was, that it becomes possible, with further therapy, to correct ‘en route’ the atrophy during the further development of the CNS so that her cerebellum would function rather physiologic at the end.

Figure 17: Cerebral palsy girl Sophie (7.5 years old) during getting up after falling and starting walking. In “A” her arms protect her when falling completely. Before being fully upright, Sophie started to walk (F).
Astonishing is that Sophie’s walking pattern was rather physiologic. The typical walking pattern of a patient with a severe cerebellum injury is completely different. Figure 18D shows the typical walking pattern of a 57-year-old patient with the loss of approximately 80% of the cerebellum and damage of the frontal (Figure 45B, C) and parietal lobe in a traumatic brain injury.
Sophie’s trot gait crawling improved. The pace gait crawling became possible with poor performance (Figure 18A). The positioning of the legs was still pathologic. The malformation was not symmetrical. To improve the walking pattern, Sophie and Nefeli exercised the walking on the knees (Figure 18B) and they liked it. Sophie’s pattern was quite physiologic apart from the abducted hands because of the balance problem. Nefeli’s arms were working fine (SCI, Th10), but her pelvis was too much backwards positioned because of trunk spasticity. After approximately 15 knee-walking steps, Sophie and Nefeli were both falling forwardly. Sophie was falling because of the loss of balance and Nefeli was falling because the spasticity which pulled her pelvic too much backward so that she was falling forwardly. But for both, the walking on knees was fun and they enjoyed the discovery of a new motor movement. Sophie could perform this movement first time in her life and Nefeli first time again after the SCI. From the therapeutic point of view this walking on knees is beneficial because it improves the walking on feet. By training parts of the walking pattern, the brain can better realize what processes are deficient in the chain of pattern events to generate the walking pattern and can correct them by learning.

Figure 18: The SCI patient Nefeli and the CP girl Sophie during crawling (A), walking on knees (B) and walking (C) in interpersonal coordination. The walking in interpersonal coordination with Nefeli helped Sophie to walk longer distances before losing balance. Note that the walking pattern of Sophie with an atrophied cerebellum and ponds was completely different to the walking of an adult patient with a severe traumatic cerebrum, cerebellum and pons injury (D).
The walking in interpersonal coordination with Nefeli (Figure 18C) helped Sophie to stay longer in the walking pattern. The stability of walking pattern improved in the short-term memory and improved in this way the learning process and contributed to the improvement of walking in general. The walking distances, quantified by the continuous steps, improved (Figure 15C). At home Sophie could now cover distances by walking instead of crawling, because with a walking distance of 5 to 10m, there was sufficient support when losing the balance. The walking pattern could therefore be used now in everyday life. As can be seen from Figure 15C, the walking improved especially with an intensive therapy of four weeks.
Cerebellum and Pons Repair through 3 years of CDT
Upgrading of the Therapy
Most of the time (11 months) Sophie exercised 8000 to 9000 turns per week on the special CDT device in the lying position (Figure 19) and trained jumping, sky walking, walking and balance (Figure 21). Mainly the balance and the higher mental functions, including the speech, improved. In the last month of therapy, the intensity was strongly increased. She exercised now approximately 50000 turns per week (9000 times per day); most of the turns were supported (Figure 19). Additionally, she trained jumping, walking and running. Real running was not possible. She could not get into the running pattern. The intensity of the therapy was therefore approximately increased by a factor of 5 to see whether more substantial repairs were possible! She trained again together with the patient Nefeli as a year before, which seemed to be beneficial for both of them. In Figure 20 she supported the training of Nefeli for fun and was improving at the same time her right-left symmetry of the arms, which is important for improving her hand and finger functions as for example the writing.

Figure 19: Sophie (cerebral palsy, malformation of cerebellum and pons) is exercising on the special CDT device, supported by her father. The father makes a small supporting mistake: his left hand has to touch Sophie’s right hand for improved input to pons and cerebellum.

Figure 20: Training of right-left coordination of arm, hand and finger functions of the cerebral palsy girl Sophie. For fun Sophie helped Nefeli with turning; but because of the coordination changes between foot paddles and handles, Sophie improved her arm and hand functions.

Figure 21: The 8-year-old girl Sophie during exercising on a special CDT device when sitting on a ball. Also balance and trunk stability were trained in this way. The younger brother Lukas was training in the background.
Improvements Achieved when exercising at her limits
After two weeks of intensive therapy, Sophie could better perform the poor pace gait crawling and she learned to walk freely on the forefoot. After 23 days of treatment a substantial repair progress occurred. The evening before she was that exhausted that she had problems to walk even with very poor performance and she slept very long. The mother was worried that Sophie may have become overloaded. But next day, Sophie wanted to jump, what she hated before, and she performed the in-phase jumping very well (Figure 22A). The performance of jumping in rotation (Figure 22AB) was good, first time in her life.

Figure 22: Sophie during jumping in in-phase (A) and in rotation (B, C).
This sudden improvement of CNS functioning can be explained by the System Theory of Pattern Formation. According to this theory, there are smooth changes with movement-based learning. But sudden changes may also occur when intrinsic (present inner CNS organization) and informational requirements (CDT) conflict, while behavioral information is changing smoothly. Such abrupt change may have taken place in Sophie in the short-term memory after approximately 6000 supported fast turns. Other movements as knee walking (Figure 23) and walking with sandals (Figure 24), which activates the forefoot, may have contributed.

Figure 23: Sophie (front) during walking on knees. A part of the pattern walking is trained in this way.
Disappointing is that the running pattern could not be learned so far. Sophie was not able to get into the high frequency pattern, even though she was able to step a bit on the forefoot.

Figure 24: Sophie (left) during walking with sandals to train forefoot functions. When Sophie and Nefeli were training together they motivated each other to fight more.
The achieved progress of the intensive CDT for 23 days was that she could jump better in-phase and learned to jump in rotation (Figure 22). Rotational movements are important to increase trunk stability and balance. It became thus possible that Sophie started by herself to perform hula hoop (Figure 25), for which trunk stability and balance is needed. The improvement of trunk stability made it possible that Sophie became able to exercise on a special CDT device when sitting on a ball (Figure 21). The activation of the forefoot could be trained now when walking with sandals (Figure 24).

Figure 25: Sophie during trying to learn hula hoop. Note the sudden rotational movements of the upper body. Trunk stability and balance are trained in this way. Astonishing is that she did not lose balance.
The most important progress achieved in the last two year was the improvement of the higher mental functions. She became able to speak more clearly, write better (Figure 40) and showed beginning of creativity, entrepreneurship and sense of initiative. She started for example to learn hula hoop by herself (Figure 25), which is no simple movement: a lot of trunk stability and balance is needed. To appreciate the progress, one has to remember that at an age of 5.5 years she was not able to walk even with support by the mother (Figure 13). The efficiency of the treatment can sometimes also be improved if the children compete with one another and can have fun together. For playing, Nefeli (11.5 years old at that time) was supporting Sophie (8 years old) and Sophie was supporting Nefeli (Figure 26). As Nefeli said afterwards, Sophie was not able to give her good rhythmic support as the Author did when he was supporting the jumping.

Figure 26: During jumping on springboard Nefeli supports Sophie (A) and Sophie supports Nefeli (B) for fun and treatment motivation.
Improvement of Coordination Dynamics Values with Therapy
A part of CNS repair is to quantify the progress. Besides clinical judgments, objective measurements are needed. The improvement of Sophie’s brain functioning by therapy was measured objectively when exercising on a special CDT device.
Figure 27 shows the improvement of the coordination dynamics at the beginning of therapy (A) and later on (B). The arrhythmicity (coordination dynamics (CD) values) reduced from 38.2 to 8.3. At the beginning of therapy (A), she got stuck with the difficult coordination’s between pace (P) and trot gait (K). Later on, she also managed well with the intermediate difficult coordination’s between pace and trot gait and could exercise rather smoothly.
Figure 28 shows the improvement of CNS functioning with ongoing therapy, quantified via the low-load CD values as measured in Figure 27. Even though children are not always trying to be good in a test, in Sophie characteristic changes were observed. When she trained intensively with up to 20 hours per week for approximately 4 weeks, the CD values got better (lower) and when she trained only 5 to10 hours per week, the values got worse. This clearly shows that an intensive therapy is much more efficient.
But why did her CD values got worse when training only with half of the load? When during development the neural networks become more complex with an enhanced connectivity, the phase and frequency coordination becomes worse. Healthy children train continuously their networks by running, jumping and other movements. The injured CNS needs not less but even more movements for holding the exactness level of phase and frequency with increasing neural network connectivity. If Sophie would have trained continuously at her limits, the CD values would vary but would not get worse.
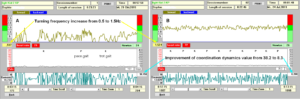
Figure 27: Coordination dynamics (CD) measurements at the beginning (A) and later on during therapy (B). The turning frequency on the special CDT device increased from 0.5 to 1.5 and the CD values reduced (improved) from 38.2 to 8.3. The cerebral palsy patient learned to exercise much better with therapy, that means more smoothly and faster.
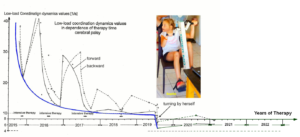
Figure 28: Low-load coordination dynamics (CD) values in dependence of therapy time in years. Forward exercising = continuous line; backward exercising = dashed line. Note, with intensive therapy periods the CD values got at each time period strongly lower (better) and successively lower. The measuring of the low-load CD values became possible, one year after the beginning of the CDT (2014), when she became able to exercise by herself on the special CDT device. The solid thick line connects the best values, which reached nearly a plateau of no further progress. When using a special CDT device with more complicated coordination’s between arms and legs, the CDT values substantially improved (lowered) further (2019). With this improvement of brain functioning, the cerebral palsy girl Sophie started to turn by herself without mental support.
Interesting is that the movements, vegetative and higher mental functions continuously improved. Most likely, if CDT would have been administered continuously at her limits, let’s say for 12 months instead of only 1 month repeatedly, then her repair would have been faster and Sophie (from Switzerland) would have had a better chance to catch-up in a few years’ time with the other healthy children of the same age. But the load on a family with a disabled child is already very high. Training then additionally at the child’s limit, in which a lot of patience is needed, may overload the family, especially when getting no help from the educational and rehabilitation systems, which are working according to duty. In Switzerland a proposal from the invalid insurance (IV) that the parents can chose the kind and place of rehabilitation was not accepted by the parliament in 2018. In the coma patient Manolis [16], who had lost approximately 50% of the brain tissue in a car accident, a miracle-like progress was achieved, when CDT was administered to him for 6 years with 20 hours therapy per week. But nearly 10 persons were contributing to the brain repair, including 2 sisters, 2 brothers and the mother. No financial support was coming from the state.
Cerebellum and pons repair within 4 years of CDT
With low-level therapy of approximately 10 hours CDT per week, Sophie improved but only little. Her handwriting improved (Figure 40, 02.06.2018) and, very importantly, her balance improved substantially. She became able to play with the father with the ball. When the balance further improved, Sophie became able to walk on the forefoot and she became able to balance the posture during ball-playing with a cousin by also going on the forefoot (Figure 29).

Figure 29: Sophie (left) with an atrophy of the cerebellum and pons during ball-playing with a healthy cousin. She trains the balance when going on the forefoot (arrow).
Still Insufficient Repair of the Vermis (Spinocerebellum)
Because of an insufficient repair of the genetical old vermis, Sophie could still not control sufficiently inertia and centrifugal forces during fast moving with the consequence that during fast creeping, she was still overstretching the legs (Figure 30a) and swinging them too much (Figure 30b) (creeping ataxia). This inability to stop leg movement on time did not improve much to the repair stage of one year ago (Figure 16B, A).

Figure 30: Sophie during creeping in interpersonal coordination in antiphase with Nefeli (SCI). Sophie is overstretching (a) and overswinging the legs (b) in comparison to Nefeli. She had not fully learned to control the inertia and centrifugal forces of leg movement. She cannot stop leg movement in time. The spinocerebellum (vermis) had not been repaired sufficiently so far.
The walking performance improved further. The overshoot of leg movement became more one-sided (Figure 31D). In the swing phase of the right leg, the stride length was not so large any more, the balance was quite good and the arms moved in coordination (Figure 31b). But in the swing phase of the left leg, the stride length was too large and Sophie had balance problems; the arms did not move in good coordination with the legs because they were used for keeping balance (Figure 31a).

Figure 31: a. During walking the left leg is over-swinging and the balance is poor; Sophie is using the arms for keeping balance. b. During the swing phase of the right leg the control of inertia and centrifugal forces is better already; she can keep balance without using the arms.
Hopefully Sophie does not have a severe atrophy of the deep cerebellar nuclei, in which case only minimal recovery is believed to occur [34]. Since the vermis is phylogenetical an older part of the cerebellum, may be some genetical old movements (as for example from the Tiktaalik’s (Figure 32)) have to be trained additionally.

Figure 32: A. Four limb walking of the monkey. Because the palm of the hand is not touching the ground, this movement is not suitable for training. B. Bear-walking of patients with brain injuries (suitable for training). C. Only the fingers and finger bones of the hands of the monkey are touching the ground. D. Tiktaalik (phylogeny between fish and Ichthyostega): the fish which is leaving the sea. Its movement on land bears similarity to push-up. E, F. Author and baby during push-up.
Upgrading of the Therapy
Figure 33 shows some movements performed with Sophie to hopefully include more efficiently the repair of the vermis (spinocerebellum). If the argument with the possible Tiktaalik’s movements is wrong, the performed movements train anyway the trunk stability, which was still deficient in Sophie. Even though Sophie could crawl very fast in trot gait coordination, the coordination of the pace gait crawling (Figure 33b) was still poor. During hopping overshoot of the right leg (Figure 33c) did occur.
To train deeper in the complexity of CNS organization, further complicated coordination’s were trained on a certain special CDT device. Sophies CNS has to recognize where there are pathologic neural network organizations and has to repair them by trial–and-error-elimination processes.

Figure 33: a. Author and Sophie during push-up. b. Pace gait crawling with Nefeli (SCI) in interpersonal coordination. As indicated, the arm of Sophie moves to late or the leg too early. c, d. Hopping movement performed with the brother Lukas. As marked, there is also dysmetria of the right foot (c) during this hopping movement.
Beginning of Running
Because of the inability to sufficiently control inertia and centrifugal forces, Sophie had problems in performing small steps. She also had problems to increase the stepping frequency. By training the increase of the stepping frequency (Figure 34a) and training volitionally to perform smaller steps (Figure 34b), she became able to learn a bit running. When moving fast with the father, she became able to run for few meters in spite of the overshoot of leg movement (Figure 34c). The training of the integrative and high frequency moving ‘running’ will, most likely, bring further repairs in Sophies CNS.
For learning running, she has to learn firstly to move with high frequency for which a precise high-speed communication between the cerebellum and the periphery is needed. Secondly, she has to learn to reduce the overshoot of leg movement. Thirdly, she has to learn to increase the pattern stability, that means to stay longer in the running pattern than just for a few running steps. Fourthly, she needs to learn running pattern variability to adapt to uneven ground. Sophie, therefore, needed to learn variability and stability of motor performance. And fifthly, she has to learn to keep balance during running. At that time, she could only get into the running pattern when she was running with the father (Figure 34c), to have support. The improvement of walking and running was in accordance with the improvement (reduction) of the low-load coordination dynamics values (Figures 27, 28).
There was still a long way of treatment to go to fully learn running. Luckily, parents, grandparents, the brother and other relations were substantially contributing to the repair of Sophies CNS.

Figure 34: a. Sophie during training high frequency stepping with the father. b. Training to reduce the stride length during walking to reduce the overshoot of leg movement (with grandparents). c. Sophie during running with the father. Note her laughing during running (c).
Improvement of Speech
The speech improved further, but it was still far away from normal. The coordination of the speaking with coordinated movements is helpful (Figure 35), since deficient speech is mainly caused by insufficient speech muscle coordination caused by cerebellum and pons atrophy.

Figure 35: Sophie during speech therapy when exercising on a special CDT device with father and mother.
Cerebellum and Pons Repair through 6 years of CDT
Through 5.5 years of CDT, Sophie learned the running. It was hard training for her, but she liked it (Figure 36B-D). By use of volitional power and intention, she got into the running pattern and could keep it for some time. The running is very efficient for repair, because the movement-induced afferent input is high (behavioral information ∑cinfFinf) in comparison to (pathologic) internal neural network organization (intrinsic dynamics Fintr). The only problem was that she got quickly exhausted.

Figure 36: B-D. The cerebral palsy girl Sophie learned through 5.5 years CDT the running. Note from the expression of the face, how hard she is fighting to run. She liked the running, even though being very hard for her. A. The SCI patient Nefeli, with whom Sophie trained partly together, lost functions with orthopedic surgery [8].
To motivate Sophie, parents and grandparents trained sometimes together with her (Figure 37). Simultaneously, they improved their own general health.

Figure 37: The patient Sophie with cerebellum and pons atrophy, during training together with the mother and the grandparents.
To further improve the running pattern performance, Sophie trained with the grandmother the forefoot activation (Figure 38). She became also able to walk and run a bit on the forefoot (Figure 38). The movements on the forefoot are important for building up the foot arc and seem to improve cerebellar functioning. When Sophie just learned to walk, the walking with sandals went astonishing well (Figure 24), probably because the toes and the forefoot were activated.

Figure 38: Forefoot training of Sophie with the grandmother during walking and running.
Through 6 years of CDT, the running performance improved and she could run longer distances with better performance. She became able to run on uneven ground (Figure 39A, B). This means that she learned to a certain degree running pattern variability to adapt to the uneven ground when the ground was too uneven, she used the arms for keeping balance (Figure 39B).

Figure 39: Cerebral palsy girl Sophie during running on uneven ground and free jumping. A. Running in normal trot gait coordination. B. When the ground was too uneven, she used the arms for keeping balance. C, D. Free jumping in pace gait coordination in front of the farther. From her face (A, B) it can be seen that she was fighting for performing running and jumping well. She liked to perform both learned movement patterns.
Also, the jumping improved. She became able to freely jump in-phase (Figure 39C, D). The jumping in anti-phase, in which she has to swing also the arms in coordination with the legs, in similarity to running (Figure 39A), she had not learned so far. Altogether, the locomotion had improved substantially. At the beginning of therapy, the farther asked the Author whether it is possible that her daughter could learn to walk up to 5m to be able to walk at home instead of covering distances by crawling. Now, Sophie walks with her cousin to a 1km distant supermarket for shopping.
In spite of the tremendous progress in movements, the cognitive functions and the fine control need further improvement through intensive CDT. The speech is still poor. The writing of Sophie improved. She became able to write better and smaller letters (Figure 40). But she did not catch-up with healthy boys and girls to visit a normal school. The integration at school may be difficult, even if Sophie would have an assistant. The spinal cord injury patient Nefeli (Figure 18) had problems with the integration at school. Pupils can be quite hard in critic. And the schools for disabled are out-of-date.

Figure 40: The cerebral palsy girl Sophie learned to combine letters to words (left) and to write at an age of 8 (13.12.2016). The writing improved when she was 9 and 9.5 years old (21.9.2017, 2.06.2018). During 6 years of CDT at an age of 12, she learned to write better and smaller letters (13.03.2021). The language is German.
The only real solution for Sophie to catch-up with healthy pupils is to further repair her CNS. But because the mainstream medicine is 30 years out-of-date, the load on the parents is high and they get worn-out with ongoing years of therapy.
Discussion
It was shown that the CNS of a young patient with an atrophy of the cerebellum and pons and may be a mild injury of the basal ganglia could substantially be repaired through Coordination Dynamics Therapy (CDT). The girl Sophie started CDT at an age of 5.5 years and could 6 years later walk run, jump and hold balance. She became continent, learned writing and her cognitive functions improved strongly.
Comparison of Therapy-Induced Improvement of CNS Functioning Between Cerebellum and Pons Atrophy and Traumatic Injury
The improvement of CNS functioning of Sophie will be compared with that of the patient Dr. Cwienk who suffered a severe traumatic brain injury at an age of 55. The frontal and parietal lobe of the cerebrum and pons were injured and 80% of the cerebellum lost. Sophie was at the beginning of therapy a severe disabled child and Dr. Cwienk was given up by school medicine. To Sophie, CDT was administered with changing intensity and Dr. Cwienk performed CDT continuously for more than 20 years with rather high intensity. Even though these two patients are quite different, still some important similarities and differences in repair will turn out.
- The most important difference between the now 12-year-old Sophie and the 80-year-old Dr. Cwienk was the speed of learning, when CDT was administered. What Sophie learned in 12 months, Dr. Cwienk needed up to 20 years.
- Sophie learned the protection automatisms when falling (Figure 17A) within 6 months and it was easy to walk with her when holding her hand. Already the walking in interpersonal coordination with Nefeli (SCI) improved her walking performance (Figure 18C). Her left arm was abducted to keep balance.
Dr. Cwienk did only re-learn the protection automatisms, when falling, after 20 years of therapy. With a lot of concentration, he could move step by step without falling (Figure 18D). But when he was really falling, it was nearly impossible to support him, because his reactions were un-physiologic and unexpected for the supporting person. It was therefore stress to support him during walking. Even the Author thought that the patient will never re-learn the protection automatisms because of the loss of 80% of the cerebellum. But he did. Therefore, what Sophie learned in 6 months Dr. Cwienk needed 20 years.
- The performance of the walking pattern was smoothly and physiologic in Sophie (Figure 17H) apart from the balance problem (Figure 18C) and the inability to stop the leg movement on time. But not in Dr. Cwienk (Figure 18D).
- Sophie could combine the getting up movement and the walking (Figure 17E-G), whereas Dr. Cwienk could not combine the two movement patterns. He first had to get up, concentrate and then start to walk very slowly step by step with support.
- Sophie could do sky-walking (Figure 41A), including sky-walking with crossed arms (Figure 41B), to activate commissural fibers (Figure 41B inset) for improving right-left communication. Quite often she overstretched the knees, what she was not doing during normal walking. This means that sky-walking is not an inborn automatism like walking. Later on, Sophie learned the sky-walking without overstretching the knees.
Sky-walking was not administered to Dr. Cwienk. But since he could walk on treadmill with both hands and one hand (Figure 41D), he could most likely also perform sky-walking because no balance is needed. Walking with sticks (Figure 41C) was already difficult for him.

Figure 41: A, B. Sky-walking of the 7-year-old Sophie with atrophied cerebellum and ponds. C, D. Walking with sticks and walking on treadmill of the 70-year-old patient with traumatic cerebellum and ponds injury. B, inset = commissural fibers of the cerebrum.
- Within 6 months, Sophie learned a bit the jumping on springboard with poor performance (Figure 14) and later on with good performance (Figure 22). The free jumping was achieved through 6 years of CDT (Figure 39). Dr. Cwienk re-learned the jumping on springboard, but the smoothness was missing. Because of extensor spasticity and missing elasticity, there was the danger of damaging the knee joints. He had no chance to learn the free jumping.
- Sophie and Dr. Cwienk re-learned the trot gait crawling, even though the performance in Sophie was better. But the pace gait crawling (Figure 18A) was difficult for both of them. The problem of Dr. Cwienk with the pace gait crawling is understandable because of his one-sided cerebellum injury (Figure 45) in some similarity to stroke. But Sophie had an atrophy of the cerebellum and not a one-sided injury. Also, the 10-year-old Nefeli (SCI) had more problems to re-learn the pace gait crawling (Figure 18A), even though during development the pace gait crawling is learned first because it is easier for the CNS to generate it.
- When being able to exercise on the special CDT device, both, Sophie and Dr. Cwienk could exercise on it in the standing position (Figure 42), because only little balance is needed.

Figure 42: Exercising on the special CDT device in the standing position of the 7-year-old Sophie with cerebellum and pons atrophy and a 60-year-old patient with traumatic cerebellum, pons and cerebrum injury. Note that when no balance is needed, both can perform this coordinated arm and leg movement, but the girl with more elegance.
- Sophie had to learn to become fully continent. Dr. Cwienk had no problems with urinary bladder functioning.
- Sophie and Dr. Cwienk had scanning dysarthria and dysarthrophonia. Both patients had also a paravermian injury/atrophy and an impaired coordination of the musculature of speech. Both patients were speaking slowly and haltingly with poor articulation. In both patients the speech improved with therapy but was still far away from physiologic after 6 years and 20 years of CDT respectively. To enhance the rate of learning/re-learning of speaking, speech therapy was partly performed when the patients were simultaneously exercising on the special CDT device (Figure 43) to improve CDT functioning in the short-term memory in general and speech performance in specific.

Figure 43: Speech therapy during exercising on the special CDT device in a girl with cerebellum and pons atrophy by the mother (A, teacher herself) and an adult patient with traumatic cerebellum and brain injury by a speech therapist (B).
- The improvement of CNS functioning in the long-term memory improved the face expression strongly in Dr. Cwienk within 10 years (Figure 43C). In Sophie the expression of the face became livelier.
- Cwienk, being 80 years old, was performing 10 hours CDT per week to keep the achieved level of repair. He had no recurrence of a colon carcinoma. Sophie was performing therapy with changing intensity. It seems that her prognosis to recover further from the atrophy of the cerebellum and pons is good, may be, in similarity to children with hydrocephalus in whom the prognosis of recovery is surprisingly good. With further therapy, further correction ‘en route’ of the development to repair the cerebellum atrophy is possible in Sophie.
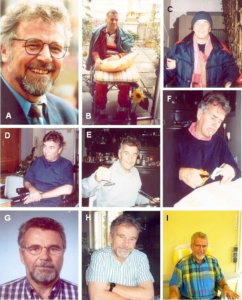
Figure 43C: Coordination dynamics therapy-induced improvement of the face expression of the patient Dr. Cwienk, who suffered severe cerebellar and cerebrum injuries. A. before the accident; B-I. After the accident in 1995 till 2006. After the injury the patient was able to move one finger. At the stage of ‘B’, his wife struggled with the physicians, because they wanted to put him to a place till he dies there. But the wife took him home and started therapy with him. Note the pathologic face expression from ‘B’ to ‘F’.
- In spite of the tremendous progress of the very intelligent Dr. Cwienk with CDT, he could not reach the high intelligence level of before the injury. As he said himself, before the injury he could listen to somebody and generate arguments against the opponent at the same time. Now, after the recovery from the severe brain and cerebellum injury, he can do only one thing at a time. This means, he first has to store the information and then develop a strategy against the arguments of the opponent. The intelligence of Sophie improved with therapy.
- Cwienk was an extremely cooperative patient, which helped him to recover partly from the severe cerebellum and frontal lobe injuries. The cooperation of Sophie was poor but improved. Her parents had to be very patient to administer therapy successfully. But when she learned a new movement, first time in her life, she used it immediately like crawling, walking on knees (Figure 18B), walking, jumping and running (Figure 39).
- The writing and drawing was poor in both patients, but improved (Figures 40, 44). For some improvement of hand coordination, Sophie needed 9 months and Dr. Cwienk a few years. After 2006 the handwriting of Dr. Cwienk got worse again due to aging, reduced therapy and not writing with the hand anymore (using a keyboard for writing). The handwriting of Sophie improved continuously with further therapy (Figure 40), including writing exercises.
The learning of continuous hand writing at school is given up in several countries. The coordination in continuous hand writing (Figure 44) between movement and cognitive functions is important for specific neural network learning and structuring the human brain and should not be given up. In aging fewer spelling mistakes are done with the continuous hand writing than with the keyboard writing. An experience made also by the Author. An interchange of letters in a word does not take place in continuous hand writing.
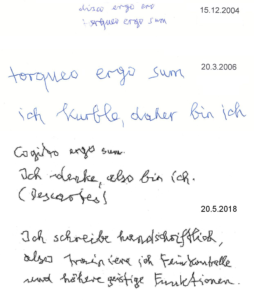
Figure 44: The writing of Dr. Cwienk. It improved within two years of CDT from 2004 to 2006. In 2018 his handwriting got worse again due to aging, reduced therapy and using only the keyboard of the computer for writing instead of performing continuous hand writing.
- No changes in the MRI with therapy could be seen for the atrophied cerebellum of Sophie (Figure 45A) and the injured cerebellum of Dr. Cwienk (Figure 45C). Repairs were mainly due to functional reorganizations. In Sophie, we can expect that some neurogenesis contributed to the repair, because CDT was started when she was 5.5 years old. In Dr. Cwienk, excitation-induced neurogenesis [35, 36] will have contributed only little because of much higher age. The building of some new nerve cells is not visible in standard MRI’s.
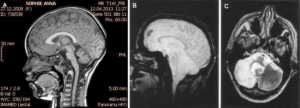
Figure 45: A. Magnetic resonance imaging of Sophie in 2013. In 2016, the cerebellum and ponds had approximately the same size, but they did not atrophy further. B, C. MRI’s of the 63-year-old patient Dr. Cwienk who suffered a severe cerebellar and cerebral injury. The cerebellum was lost/destroyed to approximately 80% (C, light parts of the cerebellum). There was also loss of brain tissue in the frontal lobe (B, dark areas) and parietal lobe (not shown). No loss of nervous tissue in the following years.
- At an age of 11 years, Sophie learned running through 5.5 years of CDT (Figure 36). Dr. Cwienk had never a chance to re-learn the free running.
- Dysmetria was very much observed in Sophie, but not in Dr. Cwienk. During crawling in trot gait coordination and walking on treadmill (Figure 41D), the Author did not see in Dr. Cwienk overshoot of leg movements due to uncontrolled centrifugal forces. But he could walk on treadmill only up to 2km and at such low-speed centrifugal forces and kinetic energies be generated only little.
- Due to a prolonged postnatal icterus in Sophie, a mild damage of the basal ganglia cannot be excluded and could have contributed to her dysmetria, because a 12-year-old boy with a damage of the basal ganglia, caused by hypoxia, showed overshoot of leg movements during walking and creeping (Figure 45A). But through CDT and ‘error-elimination processes’ (learning), also an injury of the basal ganglia can be repaired simultaneously.

Figure 45A: A boy with injured basal ganglia, caused by hypoxia, during creeping. The performance of the pattern is very pathologic (compare with Figure 30). Strong overshoot (dysmetria) of the left leg can be seen (marked). The left marked hand is also activated pathologically.
Training on the Forefoot
Some mothers of cerebral palsy patients experience that, besides the exercising on the special CDT device, the jumping on the springboard is effective for repair.
First, when jumping on springboard, the forefoot is activated. Second, the springboard has an eigen frequency of approximately 1Hz, which is the eigen frequency of a3-motoneurons (Figure 4). Therefore, when jumping on springboard, the neural network of a3-oscillators are entrained to function better. The a3-oscillators, of which the a3-motoneuronsare a part, get repaired, which can be called oscillator formation training. These a3-oscillators are self-organized through continuous jumping and building up an external loop to the periphery (Figure 46) for repair and coordination with other a3-oscillators. Third, the jumping on springboard trains dynamicity.

Figure 46: Spreading of oscillatory firing from a-motoneuron neuronal network to include muscle spindles (periphery) and synchronization of different a and g-motoneuron neuronal networks caused by touch and pin-prick stimulation.
- a-motoneuron neuronal networks fired oscillatory (solid line loop), g-motoneuron neuronal network did not or did only partly (dashed line loop), upon no additional stimulation.
- Oscillatory firing a and g-motoneuron neuronal networks built up a phase relation with muscle spindle afferents and efferents (external loop to the periphery, indicated by thick arrows) upon touch 1-5.
- (e) Oscillatory firing a (internal circuitry loop) and g-motoneuron neuronal networks (external loop) synchronized (broad peak phase relation) upon pin-pricks 6-7. The dashed line loop represents synchronization.
- (f) Oscillatory firing a (internal circuitry loop) and g-motoneuron neuronal networks (external loop) are extended by analogy from the continence muscles to muscles for locomotion. The open arrows indicate that it may be possible to synchronize spinal oscillators by rhythmic afferent input, generated by rhythmic movements (such as jumping on a springboard or running), and tore-preformat the neuronal circuitry by synapse remodeling to fire more physiologically oscillatory to reduce spasticity and improve locomotion. Extensive pathologic movement like tremor may entrain neuronal circuitry to increase tremor movement. (g) When jumping on springboard, the forefoot touches the board first. The Greek good is a bronze statue of Zeus found close to the cape of Artemision 460 BC.
Cerebellum and Pons Repair with Respect to the Ontogenetic Landscape for Locomotion
A physiologic landscape for locomotion [37] is shown in Figure 47. Because of cerebellum and pons atrophy, Sophie’s landscape for locomotion had changed.
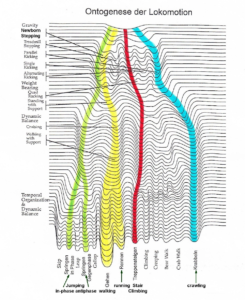
Figure 47: Ontogenetic landscape for locomotion. The evolution of the attractor layout (System Theory of Pattern Formation) for the different movements. With permission of Esther Thelen (†) [37].
CDT partly recapitulates the development. But the learning process is hampered by the deficiency of the cerebellum and pons, on which the learning process also depends. To teach the injured CNS to repair itself by trial-and-error elimination processes, the CNS has, in similarity to the development, to recognize through CDT, which subnetworks, regulation units, subloops or tracts are not functioning properly (or are missing) and to repair them by error elimination, including the possibility that other brain parts take functions partly over and subnetworks and tract fibers built anew to a limited extent.
At the beginning of CDT, at an age of 5.5 years, Sophie could only crawl in antiphase to cover distances at home by herself, whereas healthy children at that age can creep, crawl, upright, walk, run and jump. Because of missing dynamic balance, she relearned the jumping on springboard late and the running very late. The functioning of the cerebellum and pons was pathologic and too slow to be able to generate in time the patterns jumping and running, according to the ontogenetic landscape. When she eventually learned the running, her dynamic balance had improved strongly.
Ontogenetic Landscape for CNS Functioning, Quantified by the Coordination Dynamics Values, Between Healthy Children and Sophie with Cerebellum and Pons Atrophy
The learning for repair in the girl Sophie was something like 10 times faster than in the aging Dr. Cwienk. But how was the speed of learning to improve CNS functioning of Sophie in comparison to healthy children? Probably, healthy children learn much faster than the formally disabled Sophie, even though through CDT Sophie’s learning, to improve CNS functioning, speeded up. To quantify the improvement of CNS functioning in relation to healthy children, the low-load coordination dynamics values of Sophie is compared with those of healthy children.
Figure 48 shown the low-load coordination dynamics values of healthy children in the age range between 3 and 18 years when being measured the first time [15, 38]. The CD values for girls and boys were the same (Figure 49) and lumped together to have large groups, because the CNS functioning depends on many factors.
At an age range between 3 and 6 years, the healthy children had very high (poor) CD values. With ongoing development, the CD values became lower (better) and reached a plateau at an age of 18 (Figure 48, solid and dashed line). When a child was measured again, the CD values got better (dotted line), because the CNS learned to function better through the repeated measurements. If a healthy child would perform CDT, CNS functioning would improve strongly and the low-load CD values would become much lower as is shown in Figure 48 with Sophie’s brother Lukas.
Lukas, the younger brother of Sophie, was squint eyed and physicians offered spectacles. But instead of wearing spectacles, he performed for a few years CDT and the mild strabismus disappeared. Anyhow, Lukas performed for a few years low-intensity CDT and his low-load CD values became much lower than those of healthy children, not exercising on special CDT devices. If healthy pupils, therefore, would also exercise on special CDT devices during school sport, their CNS functioning would get better and they would learn faster. The female director of that gymnasium, where the pupil’s measurements were mainly done, exercised several times on a special CDT device and she liked it, because she was feeling better afterwards. She had better low and high-load CD values than the sport teacher. The sport teacher was disappointed and angry about that and blocked the use of CDT devices in school sport. At another gymnasium, the sport teacher had no problems to also use special CDT devices. In both schools (Tallinn, Estonia) also disabled pupils were attending.
The patient Sophie with cerebellum and pons atrophy had at the beginning of CDT much worse (higher) CD values than healthy pupils, measured one time (Figure 48). But with ongoing therapy, her low-load CD values became better than those of the healthy children. But, as explained with her brother Lukas, if the healthy pupils would also have trained additionally on special CDT devices for example in school sport, their low-load CD values would have become better, because of improved CNS functioning. But since Sophie’s brother Lukas could turn much better than Sophie, she had not reached the CNS functioning of the healthy girls and boys.
Some pupils of that gymnasium had less good CD values than others of same age and got depressed. The Author told them that they should not be depressed because they can improve their nervous system functioning by learning. As is shown, even Sophie could improve her nervous system functioning tremendously, quantified by CD values, through learning (Figure 48).

Figure 48: Coordination dynamics (CD) values of boys and girls (lumped together) to quantify human neural development in relation to those of the patient Sophie. The CD values, of mainly healthy pupils from a gymnasium, transiently increase at 11 years and the group size number is small at an age of 14 (puberty, missing motivation to get measured), as is indicated by arrows. The CD values for backward exercising during the whole developmental period are worse (higher). In the longitudinal study (dotted lines) CD values become smaller (better) than the average ones of the cross-sectional study due to the repeated assessment. The patient Nefeli with SCI at the level of Th10/11 has a much better (smaller) CD value because of the CDT. Approximate good CD values from Sophie and her healthy brother Lukas (mean of forward and backward exercising) are inserted according to the age. At the beginning of CDT, the CD values of Sophie are worse than the ones from healthy children. Later on, they are better. Lukas, the younger brother of Sophie, performing CDT at a low level, has much better (lower) values than Sophie and the healthy children. A value of 1.8 is the approximately the best one, one can achieve.
Frequency of Turning during Development and Repair
The frequency of turning, when exercising on the special CDT device, gives further information how much Sophie could catch up with healthy peoples. Those frequencies values were taken when the subject had the best CD value during a session. The pupils turned with their own inner frequency.
Healthy children improve their CNS functioning by movement-based learning. Such movements include running, jumping and training balance. When exercising on a special CDT device, these for the development necessary movements can be partly made visible. As can be seen from Figure 49, the children were turning generally very fast up to a frequency of 2 Hz around the age range of 9 years. Before 9 years they could not turn that fast, even though they wanted, because their neural networks were not sufficient complex to generate the complicated coordination’s between pace and trot gait. The children got stuck during turning. When being older than 9 years, they probably turned not so fast anymore, because the neural networks of the CNS did not need so much anymore the input from the fast movements. For further details of the human development with respect to CD see [1, 2, 39].
At the beginning of CDT, Sophie was not able to exercise on a special device. When she became able to turn by herself, she got often stuck, especially at the difficult coordination’s (Figure 27A), and the overall frequency of turning was low (0.5Hz). With ongoing therapy, she turned much faster (1.5Hz, Figure 27B) and nearly reached the turning frequency of the healthy pupils (Figure 49). But again, if the healthy pupils would have turned quite often, their frequency would have been even higher, because the healthy brother Lukas turned faster than all the girls and boys (Figure 49). Sophie had therefore not reached the level of CNS functioning of the healthy pupils.
In conclusion, through CDT Sophie’s CNS functioning improved very much, but she did not cache-up with healthy girls and boys.
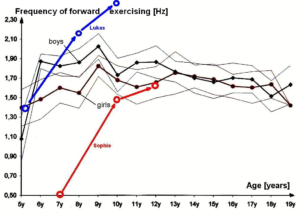
Figure 49: Frequency of forward exercising (average) of boys and girls in dependence on age. “■” are boys and “●” are girls. Note that the average group values of boys and girls are very similar. The standard deviations overlap much. The frequency of turning first increased strongly and then decreased slowly. Turning frequencies of the cerebral palsy girl Sophie and her healthy brother Lukas during their development are inserted for comparison.
Even though Sophies learning was very slow at the beginning of CDT, it speeded up with ongoing therapy. Her improved nervous system functioning will hold forever, as can be measured with low-load and high-load CD values in ageing. At an age of over 80, top athletes can still have very good low and high-load CD values! In a cerebral palsy patient like Sophie, priority has given first to the repair of the CNS through movement-based learning than the learning at school, because with the improved CNS functioning, they will learn faster afterwards.
Reasons for the Tremendous Cerebral Palsy Repair through CDT
Without CDT, the cerebellum and pons injured/malformed Sophie and Dr. Cwienk would not have improved much. Both would have lived as disabled subjects at home and may have ruined the social life of the family. In severe cerebral palsy, often fathers cannot manage the life with the disabled child and leave the family. The big load is then on the mothers with additional money problems.
But why is such great repair in cerebral palsy possible and the mainstream medicine is mainly concerned with care? The reason is that coordination dynamics therapy was developed on the grounds of human repair-neurophysiology (Method). Especially the new single-nerve fiber action potential recording method brought the progress, because it became possible to record from an ensemble of identified single afferent and efferent fibers simultaneously and analyze human nervous system functioning at the single neuron level under physiologic and pathologic conditions. Especially the phase and frequency coordination among neuron firings and its impairment could be measure with the single-nerve fiber action potential recording method (Figure 50) and the single-motor unit surface EMG (Figure 6). The human repair-neurophysiology mainly brought the progress.
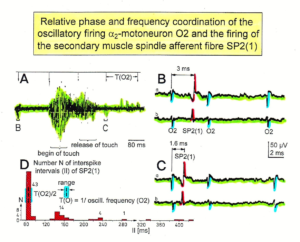
Figure 50: Time relation between the occurrence of the action potentials (APs) of the oscillatory firing a2-motoneuron O2 and the firing of the secondary muscle spindle afferent fiber SP2 (1). Brain-dead human HT6. S4 dorsal root recording. A. Overall view of the used sweep piece; only trace “a” shown. Four oscillation cycle periods of the motoneuron O2 are indicated (T (O2)). The APs of the impulse trains can be recognized only partly, because of the slow time base and poor digitalization. One impulse train (dashed arrow) is lost in the touch stimulated activity, which consists of a touch (large overall activity) and a release part (lower overall amplitude). B, C. Sweep pieces from A, time stretched. In B, motoneuron impulse train APs are marked O2, spindle afferent APs are marked SP2 (1). Note that the APs of the spindle afferent fiber are not time-locked to the first AP of the impulse train of the rhythmically firing motoneuron (relative phase coordination). D. Occurrence of inters pike intervals of the secondary muscle spindle afferent fiber SP2 (1). The numbers give the amount of IIs in each distribution peak. The oscillation period of motoneuron O2 (and the range of variation) and the half period are indicated by short dashed lines. Note that the IIs of fiber SP2 (1) are very similar to the oscillation period (or the half of it) of a2-motoneuron O2 (relative frequency coordination).
In Switzerland, insurance companies pay for care, but not for cure, even though care is on the long term more expensive. At an international conference for pediatric acquired brain injury (IPBIS2018), physiotherapists, rehabilitation physicians, neurologists and neuropediatric did not want to get informed about new developments in brain repair for children. Expert knowledge (in German: Fachwissen, Sachverstand) is not of interest anymore to the world society. No wonder that we have a Covid-19 pandemic [41]. CDT for example reduces the blood pressure [42] and improves cardio-vascular performance, so that the risk of thrombosis is reduced. Thrombosis is one side effect of Covid-19 infection/treatment.
References
- Schalow G (2002) Stroke recovery induced by coordination dynamic therapy and quantified by the coordination dynamic recording method. Electromyogr. Clin. Neurophysiol. 42: 85-104.
- Schalow G (2002) Improvement after traumatic brain injury achieved by coordination dynamic therapy. Electromyogr. Clin. Neurophysiol. 42: 195-203.
- Schalow G and Jaigma P (2006) Improvement in severe traumatic brain injury induced by coordination dynamics therapy in comparison to physiologic CNS development. Electromyogr. Clin. Neurophysiol. 46: 195-209.
- Schalow G (2003) Partial cure of spinal cord injury achieved by 6 to 13 months of coordination dynamic therapy. Electromyogr. Clin. Neurophysiol. 43: 281-292.
- Schalow G, Jaigma P, Belle VK (2009) Near-total functional recovery achieved in partial spinal cord injury (50% injury) after 3 years of coordination dynamics therapy. Electromyogr. Clin. Neurophysiol. 49: 67-91.
- Schalow G (2010) Cure of urinary bladder functions in severe (95%) motoric complete cervical spinal cord injury in human. Electromyogr. Clin. Neurophysiol. 50: 155-179.
- Schalow G (2019) Regeneration of the human spinal cord via coordination dynamics therapy. Peertechz Publications, 97 pp. eBook.
- Schalow G (2021) CNS repair in a girl with a spinal cord injury. Adv Pub Health Com Trop Med: APCTM – 121.
- Schalow G (2006) Cerebellar injury improvement achieved by coordination dynamics therapy. Electromyogr. Clin. Neurophysiol. 46: 433-439.
- Schalow G, Jaigma P (2005) Cerebral palsy improvement achieved by coordination dynamics therapy. Electromyogr. Clin. Neurophysiol. 45: 433-445.
- Schalow G (2006) Hypoxic brain injury improvement induced by coordination dynamics therapy in comparison to CNS development. Electromyogr. Clin. Neurophysiol. 46: 171-183.
- Schalow G, Pääsuke M, Ereline J, Gapeyeva H (2004) Improvement in Parkinson’s disease patients achieved by coordination dynamics therapy. Electromyogr. Clin. Neurophysiol. 44: 67-73.
- Schalow G, Nyffeler T (2001) Koordinationsdynamik-Therapie: Myelomeningozele (Spina bifida).
- Schalow G, Nyffeler T (2000) Koordinatiosdynamik-Therapie: Skoliose.
- Schalow G (2013) Human Neurophysiology: Development and Repair of the Human Central Nervous System. Nova Science Publishers, Inc, Hauppauge NY, USA, 734 pp.
- Schalow G (2019) Permanent coma patient re-learned to speak via Coordination Dynamics Therapy. Arch. Clin. Med. Case Rep. 3: 33-50.
- Schalow G (2017) Breast cancer growth inhibition via Coordination Dynamics Therapy. In: “Horizons in Cancer Research. Volume 68”. Editor: Hiroto S. Watanabe. Nova Science Publishers, Inc, Hauppauge NY, USA, pp. 125-151.
- Schalow G (2020) Anaplastic oligodendroglioma WHO III brain cancer-patient recovered following operation, radiation and chemotherapy through Coordination Dynamics Therapy, which is also a Covid-19 treatment without ventilator. Int. J. Med. Clin. Imaging 5: 165-210.
- Schalow G, Lang G (1987) Recording of Single Unit Potentials in Human Spinal Nerve Roots: a New Diagnostic Tool. Acta Neurochir. 86: 25-29.
- Schalow G (2009) The classification and identification of human somatic and parasympathetic nerve fibres including urinary bladder afferents is preserved following spinal cord injury. Electromyogr. Neurophysiol. 49: 263-286.
- Schalow G (2020) Classification and Identification of Human Peripheral Nerve Fibers by Conduction Velocity, Nerve Fiber Diameter and Natural Firing Patterns with Consequences for CNS Repair and Covid-19 Infection Treatment. Int. J. Med. Clin. Imaging 5: 231-314.
- Schalow G (2005) Phase and frequency coordination between neuron firing as an integrative mechanism of human CNS self-organization. Electromyogr. Clin. Neurophysiol., 45: 369-383.
- Schalow G (1993) Spinal oscillators in man under normal and pathologic conditions. Clin. Neurophysiol. 33: 409-426.
- Schalow G (2006) Surface EMG- and coordination dynamics measurements-assisted cerebellar diagnosis in a patient with cerebellar injury. Electromyogr. Clin. Neurophysiol. 46: 371-384.
- Schalow G (2005) Tremor in Parkinson’s disease patients can be induced by uncontrolled activation and uninhibited synchronization of α2-motoneuron firing to which α1-motoneuron firing synchronizes. Electromyogr. Clin. Neurophysiol. 45: 393-406.
- Schalow G (2010) Scientific basis for learning transfer from movements to urinary bladder functions for bladder repair in patients with spinal cord injury. Electromyogr. Clin. Neurophysiol. 50: 339-395.
- Kelso JAS (1995) Dynamic Patterns. The Self-Organization of Brain and Behavior. MIT Press, Cambridge.
- Schöner G, Zanone PG, Kelso JAS (1992) Learning as change of coordination dynamics: Theory and experiment. Journal of Motor Behavior 24: 29-48.
- Zanone PG, Kelso JAS (1992) Evolution of behavioral attractors with learning: Nonequilibrium phase transition. Journal of Experimental Psychology: Human perception and Performance, 18: 403-421.
- Popper KR (1972) Objective knowledge: An evolutionary approach. London: O.U.P.
- Touwen B (1987) Variability and stereotypy in normal and deviant development. In: Care of handicapped child. Apley, J. (Ed.). Clinics in Developmental Medicine No. 67. Philadelphia, pp. 99-110.
- Thelen E (1987) The role of motor development in developmental psychology: a view of the past and an agenda for the future. In: Eisenberg, N. (ed.): Contemporary Topics in Developmental Psychology. New York, Wiley, pp 3-33.
- Schalow G (2020) From brain repair to Covid-19 treatment via Coordination Dynamics Therapy. (Video film contains therapy movements of patients’ recent publications). Video conference August 19, 2020.
- Baehr M and Frotscher M (2005) Duus‘ Topical Diagnosis in Neurology. Thieme Verlag, Stuttgart. (a very good book for medical neuroscience since it correlates structure and function in human nervous system injuries; only human neurophysiology is missing).
- Deisseroth K, Singla S, Toda H, Monje M, Palmer TD, et al (2004) Excitation-neurogenesis coupling in adult neural stem/progenitor cells. Neuron 42: 535-552.
- Schalow G (2009) Building of New Motoneurons in the Human Spinal Cord upon Coordination Dynamics Therapy to Improve Finger Functions in Motoric Complete Cervical Spinal Cord Injury. In: Berkovsky, T.C. (Ed.), Handbook of Spinal Cord Injuries, Chapter 4. pp. 231-264, Nova Science Publishers.
- Smith LB, Thelen E (1994) A dynamic approach to the development of cognition and action. MIT Press, Cambridge.
- Schalow G (2015) Repair of the Human Brain and Spinal Cord. Nova Science Publishers, Inc, Hauppauge NY, USA, 525 pp.
- Schalow G (2015) Neural network learning in human. Nova Science Publishers, Inc, Hauppauge NY, USA, 324 pp.
- Schalow G (2021) Phase and frequency coordination improvement among neuron firing for improved CNS self-organization and neural repair in Parkinson and spinal cord injury. Int J Med Clin Imaging 6: 350-425.
- Schalow G (2020) Covid-19 infection improvement through the movement-based learning therapy ‘Coordination Dynamics Therapy’. Int. J. Med. Clin. Imaging 5: 157-164.
- Schalow G (2020) To live longer with a better quality of life through coordination dynamics therapy especially in patients with severe brain injury and brain-cancer. Int. J. Med. Clin. Imaging 5: 118-155.