Publication Information
ISSN: 2641-6859
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2018
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Coenzyme Q10 Level and Q10 Supplementation in Elite Sports: Effects on Mitochondrial Energy (Performance Fatigue) and Muscle Metabolism (Muscle Damage)
Klaus Erpenbach1*, Max C. Erpenbach1, Wolfgang Mayer2, Uwe Hoffmann3, Robert Rein3, Stefan Mücke1
1Institut für medizinische Leistungsoptimierung und Trainingssteuerung, Marienstraße 1, 50374 Erftstadt, Germany
2Lab4more GmbH Bavariahaus, Augustenstraße 10, 80333 München, Germany
3Deutsche Sporthochschule Köln, Am Sportpark Müngersdorf 6, 50933 Köln, Germany
Received Date: June 24, 2022; Accepted Date: July 08, 2022; Published Date: July 18, 2022
*Corresponding author: Klaus Erpenbach, Institut für medizinische Leistungsoptimierung und Trainingssteuerung, Marienstraße 1, 50374 Erftstadt, Germany. Email: info@im-lot.org
Citation: Erpenbach K, Erpenbach MC, Mayer W, Hoffmann U, Rein R, Mücke S (2022) Coenzymq10 Level Andq10 Supplementation in Elite Sports: Effects on Mitochondrial Energy (Performance Fatigue) and Muscle Metabolism (Muscle Damage). Adv Ortho and Sprts Med: AOASM-166.
DOI: 10.37722/AOASM.2022301
Abstract
Summary: Muscle damage and training or competition induced fatigue are the most common symptoms in elite sport impeding optimal training results or prohibiting competition. Are Q10 deficiencies responsible for these symptoms in elite sport and will daily supplementation prevent them.
Methods: In 111 elite athletes (male: 50 – female: 61) blood level of Q10 were determined. In all elite athletes performance fatigue and muscle damage were correlated. 35elite athletes were treated with daily supplementation of 400mg Q10-Emulsion for three months. Q10, cellular ATP and creatin kinase (CK) before and after supplementation were determined and muscle damage and performance fatigue symptoms were correlated.
Results: In 70% of all elite athletes (N=77/111) a blood-Q10-deficiency (<750 µg/l) was established, average levels were 653.20 ± 289.58 µg/l. In cases of young national player (U16/U18) Q10 compared to national A player were poorly supplied [Q10: 579.25 ± 233.63 µg/l vs. 751.71 ± 441.80 µg/l (p=n.s)]. Comparing the settings of Q10 < 1000µg/l vs. > 1000µg/l muscle damage were 2.34times more frequent [594 ± 190.72 µg/l vs. 1178 ± 90.85 µg/l, OR=2.34, p=0.20] in the lower group. Daily substitution of 400mg Q10-Emulsion improved Q10-level in blood significantly (670.57 ± 273.08 µg/l before vs. 2399.29 ± 810.49 µg/l after supplementation, p<0.001), significantly optimized cellular ATP (92.21 ± 10.02 %T-cells before vs 99.11 ± 1.05 %T-cells after supplement-ation, p<0.001) and significantly reduced muscular CK levels (444.76 ± 239.61 U/l before vs 265.71 ± 156.75 U/l after supplementation, p<0,01). Female athletes showed signifi-cantly greater blood levels of Q10 than male athletes (female: 725.73 ± 73 µg/l vs male: 645.29 ± 258.09 µg/l, p<0.01).
Athletes suffering from muscle damage showed higher levels of CK than athletes without muscle damage (CK: 684.95 U/l muscle damage vs 250 µg/l without muscle damage). A significant absolute risk reduction of 68.6% for muscle damage (26/35 before vs 2/35 after therapy, p<0.0001) and of 51.4% for performance fatigue (21/35 before vs 3/35 after therapy, p<0.0001) were found. No side effects were observed.
Conclusion: Independently to the type of sports, deficiency of Q10 in blood in elite sports was observed. Daily Q10 substitution can significantly reduce performance fatigue and muscle damage by optimizing mitochondrial ATP-energy-metabolism. Randomized treatment trials over a whole season should be performed to determine whether performance fatigue or muscle damage could be avoided through daily Q10 substitution.
Introduction
Micronutrients – vitamins and trace elements – are essential and daily necessary to optimally maintain all physiological body functions [1-2]. High training intensity, tight game schedules, unbalanced or improper diets, frequent travel and permanent psychological stress lead to enormous consumption of these micronutrients resulting in injuries in 12.9% of cases and acute infections in 9.2% of cases, ending in termination of training and competition cancellations [3-6]. In major events (Olympic Games, FIFA World Cup, IAAF) 9.6-14% of participants drop out of competition due to injuries [5-13]. Similar, 5.4-8.9% of participants suffer from acute infectious disease, thereby prevalence is twice as often during winter compared to summer periods [5-13].
During performance, coenzyme Q10 (Q10) is a fundamental catalyst necessary for cellular energy production. Q10 can be produced in the human body and occurs in skeletal and cardiac muscle tissues as well as in the liver, kidney, and the brain [14]. Physical activity increases metabolic activity and oxygen consumption and thus the production of reactive oxygen causing muscle fatigue and corresponding oxidative damage. Q10 increases energy production in muscle mitochondria increasing muscular performance and reducing fatigue [15]. Q10 functions as the main part of the mitochondrial respiratory chain and therefore is an important link to cellular energy production [16]. The aim of this study was therefore to determine Q10 blood levels in elite athletes, to study possible correlations between muscle injury and performance fatigue in elite athletes and to reduce muscle damage and performance fatigue through daily Q10 supplementation.
Methods
In total, 111 elite athletes from different sports (team sports: field hockey, soccer – individual sports: athletics, tennis, motor sports) were included into the study cohort. All athletes gave their written consent to participate in the study. A questionnaire was used to assess the frequency of medically confirmed muscle-tendon injuries (muscle-fiber as well as muscle-bundle tears and tendon-muscle tears) and performance fatigue defined as physical exhaustion immediately after training/competition (in the Visual Analog Scale > 5) with persistent morning fatigue after 7-hour sleep. Blood Q10 levels were determined in all 111 athletes and correlated with muscle injury and performance fatigue symptoms. In an observational study 35 elite athletes were substituted with daily 400mg Q10 emulsion (Bionovelia Q10R, Fagus Pharma, Brühl, Germany) for three months. Blood Q10, cellular ATP and creatine kinase (CK) were determined before and after therapy and correlated with muscle injury and performance fatigue symptoms in the cohort.
Coenzyme Q10 (serum)
The determination of Q10 in serum was performed via high performance liquid chromatography (HPLC) using a commercial kit (Chromsystems, Gräfelfing, Germany) according to the manufacturer’s instructions (Q10 – OrderNo.68000).
Creatine kinase (serum)
Creatine kinase in serum was determined using an Abbott Alinity C automated laboratory kit according to manufacturer’s instructions (order no. 8P4220).
Mitochondrial Function via Mitochondrial Membrane Potential (ATP Level)
PBMC fraction was isolated from heparinized blood by Ficoll density gradient centrifugation and taken at a concentra-tion of 1million PBMCs/ml in RPMI medium containing 5% serum. Measurements were performed using the Cell Meter™ JC-10 Mitochondrial Membrane Potential Assay Kit optimized for flow cytometry from ATT Bioquest (Catalog number: 22801) according to the manufacturer’s instructions on a FACS Calibur from Becton Dickinson. The dye JC-10, derived and optimized from JC-1, binds selectively in the mitochondrial membrane and changes its fluorescence spectrum from orange to green with decreasing membrane potential. The membrane potential can be considered as a direct summation marker and endpoint for ATP production. As read out, the percentage of T cells (CD3+) without reduction of membrane potential was recorded (“ATP level”).
Statistical Analysis
All statistical analyses were performed using R software package (version 4.1.2). Group comparisons were tested using a mixed linear model. Gender and age were included as covariates in the model while participant differences were modeled as random effects. In case of statistically significant main effects, differences were tested by post-hoc tests based on corrected marginal means and Tukey correction for multiple testing. The conditions for inference of statistical effects were checked using quantile-quantile plots of model residuals. Statistically significant effects for 2×2 frequency tables for muscular and general fatigue were checked using McNemar tests. The level of statistical significance was set at α = 0.05 for all tests. Therefore, for p ≤ 0.05, the results were considered statistically significant, or highly significant for p ≤ 0.01. Effect sizes were calculated according to Cohen’s d when appropriate and interpreted following the usual classification (< 0.2 small, 0.2 < 0.5 medium, > 0.5 large).
Results (n=111) ± 7,43 ± 289,58 (n=111) (n=61) ± 6,16 ± 241,12 (n=60) (n=50) ± 8 ± 340,93 (n=50) (n=21) ± 4,05 ± 468,48 (n=20) (n=62) ± 4,62 ± 217,25 (n=62) Participants (n=19) ± 10,86 ± 291,55 (n=19) (n=5) ± 6,5 ± 254,55 (n=5) (n=4) ± 6,85 ± 148,08 (n=4) (n=27) ± 5,35 ± 420,2 (n=27) (n=6) ± 0,82 ± 187,26 (n=6) (n=15) ±0,64 ± 241,6 (n=15) (n=6) ± 0,9 ± 241,6 (n=6) ± 289,58 (N=111) Adults ± 441,80 (N=24) U16 – U18 ± 233,63 (N=24) ± 275,72 (N=21) Adults ± 289,58 (N=42) 750-1200 µg/l N=35 N=24 N=11 pre Fatigue post ARR Significance (60%) 3/35 (8,6%) 51,4% p<0,0001 (50%) 1/24 (4,2%) 46,8% (81,8%) 2/11 (18,2%) 53,6% pre Muscle Injury post ARR Significance (74,3%) 2/35 (5,7%) 68,6% p<0,0001 (75%) 2/24 (8,3%) 66,7% (72,7%) 0/11 (-%) 72,7% pre Q10 post Significance ± 273,08 2399,29 ± 810,49 p<0,001 ± 258,09 2175,29 ± 593,97 ± 308,96 2888,00 ± 1019,23 pre ATP post Significance ± 10,02 99,11 ± 1,05 P<0,001 ± 8,53 99,17 ± 1,08 ± 12,36 98,96 ± 1,04 pre CK post Significance ± 239,61 265,71 ± 156,75 p<0,01 ± 261,35 284,57 ± 163,62 ± 84,48 177,67 ± 91,85
(Table 1) shows the blood Q10 levels of the study population subdivided by sex, age and type of sport. 44% of the athletes complained of performance fatigue and 73% muscle injury. In the total population, the mean blood value of Q10 was 653.21 ± 289.58 µg/l, but only 70% of the performance athletes (N=77/111) showed confirmed Q10 deficiency (< 750 µg/l). (Table 2) shows the comparison of the blood Q10 levels of youth vs. adults. Young athletes were worse supplied with Q10 compared to adults [U16/18: 579.25 ± 233.63 µg/l vs. national A athletes: 751.71 ± 441.80 µg/l (p=n.s)]. In Q10 group comparison (< 1000µg/l vs > 1000µg/l Q10 in serum), muscle injury was 2.34 times more frequent in the group < 1000µg/l blood Q10 level [594 ± 190.72 µg/l vs 1178 ± 90.85 µg/l, OR=2.34, p=0.20] than in the group > 1000µg/l blood Q10 level (Table 3). Daily substitution of 400mg Q10 emulsion for 3 months significantly increased serum Q10 (670.57 ± 273.08 µg/l before vs. 2399.29 ± 810.49 µg/l after therapy, p<0.001) (Table 4). Cellular ATP increased significantly (92.21 ± 10.02 %T cells before vs 99.11 ± 1.05 %T cells after therapy, p<0.001), while muscular CK was significantly reduced (444.76 ± 239.61 U/l before vs 265.71 ± 156.75 U/l after supplementation, p<0.01) (Table 4.). Female athletes (female: 725.73 ± 73 µg/l vs male: 645.29 ± 258.09 µg/l, p<0.01) had significantly higher blood Q10 level than male athletes (Figure 1). Athletes with muscle injuries had a higher blood CK level than athletes without muscle injuries (CK: 684.95 U/l with muscle injuries vs 250 µg/l without muscle injuries) (Figure 2). A significant absolute risk reduction in muscle injury of 68.6% (26/35 before vs 2/35 after therapy, p<0.0001) and in performance fatigue of 51.4% (21/35 before vs 3/35 after therapy, p<0.0001) was calculated in the treated athletes (Figure 3). The athletes reported no side effects.
Age
Q10
750-1200
µg/l
Total
22,34
653,2
Female
20,13
642,7
Male
25,04
665,8
Soccer
22,9
703,6
Field-Hockey
19,37
623,6
Olympia-
29
721,8
Tennis
21,6
638,8
Motor
34,75
552,5
National
23,59
738,3
U16
13,67
496,7
U18
16,47
602,1
U21
18,78
618,7
Qu10
750-1200
µg/l
Total
653,21
National Player
751,71
National player
579,25
Other U18
592,05
Other
668,31
Probands
Q10
A
≤ 1000
B
> 1000
n
Total
600
102
± SD
± 187,33
Total
1328
8
± SD
± 488,27
Performance Fatigue
yes (A)
635
45
± SD
± 193,34
yes (B)
1123
4
± SD
± 98,17
OD=0.99 – p=0,625
no (A)
573
57
± SD
± 179,55
no (B)
1533
5
± SD
± 659,11
Muscle injury
yes (A)
594
76
± SD
± 190,72
yes (B)
1178
5
± SD
± 90,85
OD=2,34 – p=0,197
no (A)
618
26
± SD
± 179,45
no (B)
1478
4
± SD
± 698,37
Total
Male
Female
Fatigue
21/35
12/24
9/11
Muscle Injury
26/35
18/24
8/11
Q10
670,57
645,29 *
725,73 *
ATP
92,21
93,85
88,80
CK
444,76
459,14
377,67

Figure 1: Q10 level and standard error before and after therapy with 400mg Q01 emulsion daily for 3 months (N=35), male (N=24), female (N=11). *** = p<0.0001 # = p<0.01.
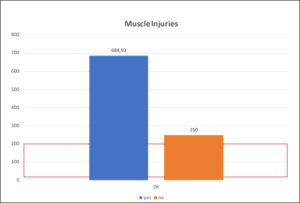
Figure 2: Creatine kinase (CK) levels in athletes with (blue bar) and without muscle injury (orange bar) before Q10 substitution (n=17). Red frames = normal range (30-200 U/L).
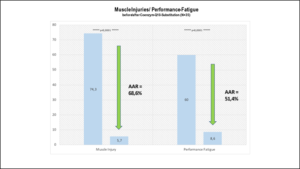
Figure 3: Absolute risk reduction (AAR) of muscle injury and performance fatigue after 3 months of Q10 supplementation.
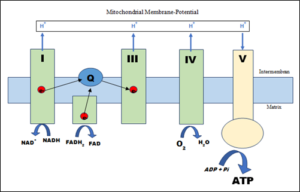
Figure 4: Q10-dependent ATP metabolism in the muscle cell mitochondrion. I-V = complexes of the respiratory chain – Q = coenzyme Q10 – e- = electron – NAD = nicotinamide adenine dinucleotide – FAD = flavin adenine dinucleotide.
Discussion
The prevalence of a blood Q10 deficiency (70% of all athletes< 750µg/l) in our study is unique so far. The median Q10 blood level of international studies – 850 µg/l [17] and 1355 ± 189.93 µg/l (18) [N=33] – are different to the median Q10 blood level in our study (N=111): 653 ± 289.58 µg/l. U16/U18 national players (579.25 ± 233.63 µg/l) had a significantly lower blood Q10 level than the A-team national players (751.71 ± 441.80 µg/l). Adolescent athletes suffering from a blood Q10-deficiency (< 750 µg/l) are more frequent compared to adult athletes (79,1% vs. 63.2% – OR = 2.20 – p<0.078). Q10 is fundamental in the mitochondrial respiratory chain for energy production (ATP) and protein synthesis in the citrate cycle: a possible reason for the higher amount of Q10 deficiency in adolescents (increased mitochondrial energy necessary for cell proliferation during growth) and the high number of muscle injuries in adolescent athletes in our study (U16/ U18 national players vs adolescent athletes< 18 years of age: 83% vs. 87% vs. 73%). Blood Q10 level was lower in athletes with muscular injuries (623.31 ± 226.31 µg/l) than in athletes without muscular injuries (732.93 ± 408.19 µg/l). All these data in our study are unique so far and suggest that closer monitoring of Q10 blood level may be advantageous and necessary in elite athletes. Comparing the prevalence of muscular injury and performance fatigue in athletes with Q10 levels > 1000 µg/l versus athletes with Q10 levels < 1000 µg/l, Q10 levels < 1000 µg/l are 2.34 times higher to suffer from muscular injury than athletes showing blood Q10 levels > 1000 µg/l (OR=2.34 – p<0.197). Blood Q10 levels in our observational treatment study confirm the blood Q10 level of competitive athletes in the cohort study (observational study: 670.57 ± 273.08 µg/l – cohort study: 653.21 ± 289.58 µg/l). Daily substitution with 400mg Q10 emulsion increased blood Q10 levels significantly after 3 months (670.57 ± 273.08 µg/l pre vs. 2399.29 ± 810.49 µg/l after therapy, p<0.001), resulting in significantly increased mitochondrial ATP production (92.21 ± 10.02 %T cells before vs 99.11 ± 1.05 %T cells after therapy, p<0.001) and thus improved muscular metabolism (CK: 444.76 ± 239.61 U/l before vs 265.71 ± 156.75 U/l after supplementation, p<0.01). Kon et al [17] achieved in a placebo-controlled therapeutic study (N=18 kendo athletes – daily 300mg Q10 for 3 weeks) a significant increase in Q10 levels compared to athletes taking placebo (verum: 850 µg/l to 4000 µg/l vs placebo: 855 µg/l to 865 µg/l – p<0.01) and a significant decrease in CK activity during the training camp (verum: from 255 U/l to 830 U/l vs. placebo: 260 U/l to 1500 U/l – p<0.05).
Improved oxidative phosphorylation in the mitochondrial respiratory chain (Q10-dependent) and thereby decreasing muscular lactate production (longer optimized aerobic exercise phase) possibly lead to this decrease in CK levels (muscular enzymes in micro injuries) [17, 18]. Demirci et al [18] confirmed these results in their placebo-controlled study. 15 athletes were divided into 3 groups (placebo – daily 100mg Q10 – daily 200mg Q10 over 1 week training camp). In the substitution group, blood Q10 levels increased significantly in the verum groups compared to the placebo group (100mg: 1570 ± 220 µg/l to 2240 ± 730 µg/l vs. 200mg: 2120 ± 320 µg/l to 3800 ± 540 µg/l vs. placebo: 1570 ± 560 µg/l to 1500 ± 270 µg/l – p<0.01) within 1 week substitution [18].
Achieving blood Q10 optimization, a significant CK activity reduction was demonstrated in the verum groups compared to the placebo group (100mg: 131.4 ± 8.01 U/l to 583.6 ± 9.86 U/l vs. 200mg: 129 ± 2.01 U/l to 499.6 ± 13.3 U/l vs. placebo: 135 ± 15.6 U/l to 648.4 ± 19.5 U/l – p<0.001). Mitochondrial function (lactate dehydrogenase = LDH) was preserved within Q10 substitution (100mg: 146.2 ± 13.7 U/l to 271.4 ± 11.2 U/l vs. 200mg: 118 ± 12.9 U/l to 240.9 ± 9.24 U/l vs. placebo: 151 ± 12.9 U/l to 442.6 ±32.4 U/l (norm < 250 U/l) – p<0.001). Maintaining optimal mitochondrial oxidative phosphorylation under Q10 substitution, lactate accumulation was significantly lower during training camp (100mg: 2.59 ± 0.26 mmol/l to 1.21 ± 0.33 mmol/l vs. 200mg: 2.37 ± 0.37 mmol/l to 0.55 ± 0.16 mmol/l vs. placebo: 2.15 ± 0.12 to 4.40 ± 0.66 mmol/l – p<0.01) [18,20]. Alf et al [19] demonstrated a significant increase in performance (verum: 11.03% vs. placebo: 8.54% – p=0.03) in a placebo-controlled study of 100 German Olympic athletes (placebo vs. 300mg Q10 daily for 6 weeks). Gharahdaghi et al [21] confirmed the effectiveness of performance enhancement in professional soccer players in a placebo-controlled therapeutic study. Daily administration of 300mg Q10 for 4 weeks increased VO2max(ml/kg/min) [verum: 52.27 ± 3.21 before to 53.63 ± 2.54 after therapy vs placebo: 51.28 ± 1.88 before to 50.80 ± 2.24 after therapy – p=0.003], vVO2max (km/h) [verum: 16.40 ± 1.26 before to 17.00 ± 1.15 after therapy vs placebo: 15.83 ± 2.04 before to 15.66 ± 0.81 after therapy – p<0.05] and performance test (Hoff Test in m) [Verum: 1374.40 ± 95.13 before to 1421.50 ± 72.61 after therapy vs Placebo: 1361.66 ± 30.76 before to 1342.16 ± 35.55 after therapy – p<0.05] were significantly increased compared to placebo-treated participants [21].
Further therapy studies substituting 300 – 400 mg Q10 emulsion are needed to show whether target blood Q10 levels in the range of 2500 – 4000 µg/l reduce or prevent muscular injury and increase performance status of the athletes and reduce performance fatigue, respectively.
Conclusion
Elite athletes may often display a deficient in Q10 blood level. Adolescents < 18 years of age are more deficient in blood Q10 levels than adults. Daily administration of 400mg Q10 emulsion optimizes blood Q10 levels, improves mitochondrial energy production ATP and lowers muscular creatine kinase preventing muscle damage and reducing performance fatigue. Further randomized studies treating elite athletes a complete season of competition to reach permanent blood Q10 level in an adequate range of 2500 – 4000 µg/l Q10 have to show whether a complete reduction of performance fatigue or muscular injury and additionally an increase in performance can be achieved.
References
- Rodriguez NR, DiMarco NM, Langley S (2009) American College of Sports Medicine position stand. Nutrition and athletic p Med Sci Sports Exerc 41: 709-731.
- Kreider RB, Wilborn CD, Taylor L, Campbell B, Almada AL, et al. ISSN exercise & sport nutrition review: research & recommendations. J Int Soc Sports Nutr 2010; 7:1-43.
- Walsh NP, Gleeson M, Shephard RJ (2011) Position Part one: immunefunction and exercise. Exerc Immunol Rev 17: 6-63.
- Gleeson M, Pyne DB (2016) Respiratory inflammation and infections in high-performance Immunol Cell Biol 94:124–131.
- Junge A, Engebretsen L, Mountjoy ML, Alonso JM, Renström PAFH, et al. (2009) Sports injuries during the SummerOlympic Games 2008. Am J Sports Med 37: 2165-2172.
- Engebretsen L, Steffen K, Alonso JM, Aubry M, Dvorak J, et al. Sports injuries and illnesses during theWinter Olympic Games 2010. Br J Sports Med 44: 772-780.
- Engebretsen L, Soligard T, Steffen K, Alonso JM, Aubry M, et al. (2013) Sports injuries and illnesses during theLondon Summer Olympic Games 2012. Br J Sports Med 47: 407-414.
- Soligard T, Steffen K, Palmer-Green D, Aubry M, Grant ME, et al. (2015) Sports injuries and illnesses in the Sochi2014 Olympic Winter Games. Br J Sports Med 49: 441–447.
- Junge A, Dvorak J, Graf-Baumann T (2004) Football injuries during the World Cup 2002. Am J Sports Med2004 32: 23S–27S.
- Dvorak J, Junge A, Grimm K, Kirkendall D (2007) Medical report from the 2006 FIFA World Cup Germany. Br J Sports Med 41: 578-81.
- Alonso JM, Tscholl PM, Engebretsen L, Mountjoy M, Dvorak J, et al. Occurrence of injuries and illnesses during the 2009 IAAF World Athletics Championships. Br J Sports Med 44: 1100-1105.
- Alonso JM, Edouard P, Fischetto G, Adams B, Depiesse F, et al. (2012) Determination of future prevention strategiesin elite track and field: analysis of Daegu 2011 IAAF championships injuries and illnesses surveillance. Br J Sports Med 46: 505-514.
- Alonso JM, Jacobsson J, Timpka T, Ronsen O, Kajenienne A, et al. (2015) Preparticipation injury complaint is a riskfactor for injury: a prospective study of the Moscow 2013 IAAF championships. Br J Sports Med 49: 1118-1124.
- Kei M, Tanaka M, Nozaki S, Mizuma H, Ataka S, et al. (2008) Antifatigue effects of coenzyme Q10 during physical fatigue. Nutrition 24: 293–299
- Witt EH, Rezhick AZ, Viguie CA, Starke-Reed P, Packer L (1992) Exercise, oxidative damage and effects of antioxidant manipulation. J. Nutr 122: 766-773.
- Frederick L, Crane PD (2001) Biochemical functions of coenzyme q10. J Am Coll Nutrition 20: 591-598.
- Kon M, Tanabe K, Akimoto T, Kimura F (2008) Reducing exercise-induced muscular injury in kendo athletes with supplementation of coenczyme Q10. Brit J Nutr 100: 903-909.
- Demirci N, Beytut E (2014) Effects of oral coenzyme Q10 on preventing the accumulation of lactic acid developing during the exercise performances of endurance skiing athletes. Am J Sports Sci 2: 65-70.
- Alf D, Schmidt ME, Siebrecht S (2013) Ubiquinol supplementation enhances peak power production in trained athletes: a double blind, placebo-controlled study. J Int Soc Sports Nutr 10: 24
- Erpenbach K, Mücke S (2017) Mitochondriale Ernährung. Sportärztezeitung 4: 88-91.
- Gharahdaghi, N, Shabkhiz F, Azarboo E, Keyhanian A (2013) The Effects of Daily Coenzyme Q10 Supplementation on VO2max, vVO2max and Intermittent Exercise Performance in Soccer Players. Life Science Journal 10: 22-28.
