Publication Information
ISSN: 2688-0873
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2018
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Archives |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Case Report: Gastric Volvulus Revealed by Peritoneal Syndrome
Elloumi*, H. Harbi, MT. Frikha, R. Mzali
Visceral and digestive surgery department, Habib Bourguiba Hospital, Sfax, Rue Al Firdaws, 3029, Tunisia
Received Date: April 10, 2021; Accepted Date: May 10, 2021; Published Date: May 20, 2021
*Corresponding author: H.Elloumi, Visceral and digestive surgery department, Habib Bourguiba Hospital, Sfax, Rue Al Firdaws, 3029, Tunisia. Email: habibledoc@gmail.com
Citation: Elloumi H, Frikha MT, Mzali R (2021) Case Report: Gastric Volvulus Revealed By Peritoneal Syndrome. Jr Surg Opetech Anesthesia: JSOPA-114.
DOI: 10.37722/JSOTA.2020101
Abstract
Acute gastric volvulus is a diagnostic and a therapeutic emergency; it can be complicated by peritonitis and gastrointestinal bleeding. 43-year-old Mrs. R.M is reported with a history of adrenal insufficiency and hypothyroidism, who consults for sudden abdominal pain as well as unproductive vomiting. The examination notes abdominal distension and polypnea, the biology marks a SIB and acute renal failure. The computed tomography examination reveals a large abundance of pneumoperitoneum and partial gastric pneumatosis. The patient was operated on for peritonitis related to gastric perforation resulting from a complete mesenteric-axial volvulus of the stomach; we also note the presence of a wandering spleen during exploration. The patient underwent mechanical resection of the necrotic peripheral portion of the stomach. The course was marked by the onset of septic shock, acute adrenal insufficiency and the death of the patient on D-3 postoperatively.
Keywords: Gastric perforation; Gastric volvulus, management; mesenteric-axial
Introduction
Gastric volvulus is a rare condition, the incidence of which is difficult to estimate. In 5% of cases this pathology is revealed by a complication [1]. In acute and complicated forms, diagnosis and treatment should be carried out urgently [2, 3]. The clinical and therapeutic peculiarities of a case of gastric volvulus revealed by acute peritonitis are reported.
Observation
This is a 43-year-old female patient with a medical history of adrenal insufficiency and treated hypothyroidism. She presented multiple episodes of vomiting progressing by seizures and giving way spontaneously for a year. She has been presenting for 3 days for epigastric pain associated with nausea and not giving way to medical treatment. Faced with the worsening and generalization of pain throughout the abdomen, she went to the emergency room.
Clinical examination of the patient found blood pressure at 90/60 mm Hg, pulse at 110 bpm, polypnea at 32 C / min, and generalized abdominal distension with defense of the left hypochondrium. A Biologically, she had a hyperleukocytosis at 18,000 elements / mm3, an elevated CPR at 380 mg /l and acute renal failure (renal clearance at 25 ml / min).
The patient was admitted to a surgical intensive care unit. She had monitoring measures, crystalloid filling, ventilation with a mask, a nasogastric tube which brings back a bilious fluid and a preparation for the realization of an emergency surgical treatment…
An unprepared x-ray of the abdomen showed gastric gas distension and parietal emphysema of the stomach (Figure 1).
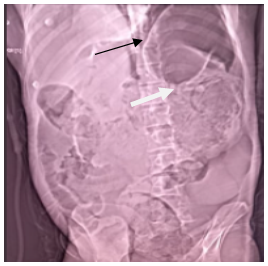
Figure 1: Abdomen without preparation revealing pneumoperitoneum (black arrow) and thickening of the gastric wall (white arrow).
The abdominal CT scan found fluid effusion and extensive pneumoperitoneum as well as partial gastric pneumatosis (Figures 2, 3 and 4).
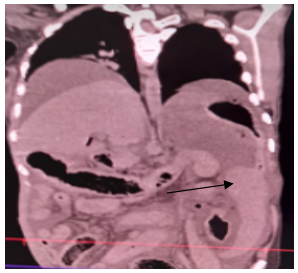
Figure 2: Frontal section of a thoraco-abdominal CT scan showing an ectopic position of the spleen tilted down (black arrow).
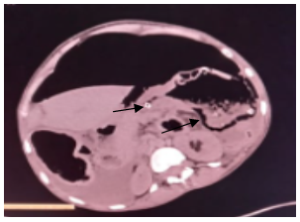
Figure 3: Axial section of an abdominal CT scan showing parietal emphysema in the volvulated portion of the stomach (black arrow).
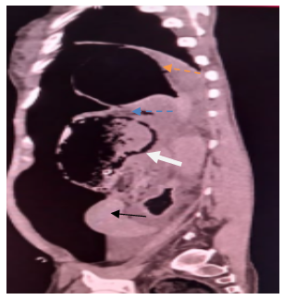
Figure 4: Coronal slice of an abdominal CT scan showing the site of the stomach volvulus (blue arrow), parietal pneumatosis (white arrow).
In addition, the proximal gastric portion (orange arrow) is healthy and the spleen is in an ectopic position (black arrow).
After a brief resuscitation, the patient was operated on by the midline. There was generalized purulent peritonitis and complete mesenteric-axial stomach volvulus resulting in peripheral gastric necrosis that follows all around the greater curvature and part of the fundus. In addition, there was a 2 cm posterior perforation of the necrotic portion. The spleen was very mobile (wandering spleen) with hyperlaxity of the gastro-splenic and gastro-phrenic ligaments (Figures 5 and 6) with the possibility of easily lowering the cardia more than 10 cm from the esophageal hiatus.
 Figure 5: Intraoperative appearance of gastric necrosis.
Figure 5: Intraoperative appearance of gastric necrosis.
 Figure 6: Intraoperative appearance of gastric perforation.
Figure 6: Intraoperative appearance of gastric perforation.
The patient underwent peritoneal toilet and longitudinal gastrectomy removing the entire necrotic portion of the stomach. This was achieved by linear stapling forceps as in the case of a sleeve gastrectomy. The remaining stomach was relatively large and not tubular. The postoperative course was marked by the onset of acute adrenal insufficiency and a state of septic shock leading to the death of the patient on D-3 postoperatively.
Discussion
Gastric volvulus is defined by an abnormal rotation of all or part of the stomach with respect to one of its axes causing upper digestive stenosis with the risk of strangulation [4, 5]. This is a rare condition given the stomach’s ability to fixate [6]. It is usually seen in people in their 50s [4, 5], although cases have been reported in younger subjects like our patient [1, 7]. In the literature, there is no gender predilection [2, 4] although some authors believe that there is a female predominance [3, 8]. Several etiologies of LV have been suggested: diaphragmatic hernias are the most frequent cause [2, 9]. “Wandering spleen” or “beating of the bell” spleen can also be another common cause of LV. Indeed, the absence of the gastro-splenic ligament and the posterior fixation of the meso of the spleen tilts the great curvature and the posterior face of the stomach forward as was the case of our patient [10-12]. We also cite liver abnormalities and gastric tumors [9, 13]. Ligament hyperlaxity is a constant and essential element favoring the occurrence of LV. It causes the posterior surface of the stomach to tilt forward, starting the first stage of a volvulus. It can be congenital or acquired (eg due to pregnancy, obesity, dehydration or muscle atrophy) [10, 16-18]. There are four types of LV : organo-axial rotations (along a cardio-pyloric axis) which are the most frequent (> 60%), mesenteric-axial rotations (along a medio-gastric transverse axis passing through the small and the large curvatures) which are seen in 29% of cases, combined or mixed rotations (10%) and the so-called unclassifiable type (2%) [14]. Organoaxial type volvuli are often described in hiatus hernias and antrum tumors [14, 15].
LV is said to be complete when the angle of rotation of the stomach is between 180 ° and 360 ° with gastric obstruction and strangulation. LV is said to be incomplete when the rotation is less than 180 ° [14]. LV can present in an acute, subacute or chronic clinical form: in the chronic form, the symptoms are not very specific, not very noisy with an evolution by crises giving way spontaneously and suddenly [21]. The subacute form is the prerogative of mesenteric-axial forms such as our case with signs related to gastric emptying disorders [21]. The acute form is characterized by the classic Borchart triad associating acute epigastric pain. (And / or left hypochondrium), abdominal distension and nausea [1]. In the absence of this triad, the acute form can be revealed by a complication, namely mainly a high digestive stenosis of sudden installation, a gastric perforation (secondary to gastric strangulation and at the origin of peritonitis) or a hemorrhage upper digestive system [1, 19, 21]. Other complications of LV can be mediastinitis, cardiac arrhythmias, tamponade, and respiratory distress [1].
Our observation is a case of acute gastric volvulus with a history of subacute attacks, associated with ligament hyperlaxity and a wandering spleen, who consults for a Borchart triad and peritoneal syndrome evolving for three days. X-ray of the abdomen without preparation is generally not helpful but can sometimes show gas distension of the upper abdomen or parietal emphysema [20], as was the case in our observation. Thoraco-abdominal computed tomography is the gold standard: it makes it possible to make a positive diagnosis of LV, to specify the type of rotation and to look for a possible complication, mainly gastric parietal necrosis (and / or vascular suffering). It also makes it possible to highlight an associated gastric tumor or a wandering spleen [6]. LV is a surgical emergency because it requires rapid stomach distortion and gastropexy [6, 22]. This can be done by laparotomy or by laparoscopy [3, 6, 22, 23] knowing that the laparoscopic technique offers the classic advantages of a shorter hospital stay and less morbidity [22-24]. The causes of conversion (10%) are dominated by the presence of ischemia and the difficulty of exposure [3, 25, 26]. The treatment in case of necrosis or perforation consists in performing a gastrectomy, which is exceptionally complete [2] as we did in our patient who had a longitudinal gastrectomy removing the necrotic part.
The postoperative morbidity and mortality of acute forms of LV is relatively high: the morbidity exceeds 66% and is favored by the oragano-axial type of rotation, complete obstruction and the presence of cardio-respiratory defects [3, 26, 27]. Mortality rises to more than 50%. The factors of poor prognosis are advanced age, the presence of comorbidities, the urgency of the surgery, the presence of necrosis requiring gastric resection and the delay in diagnosis and treatment [28 -30]. Our patient was young, but had all the other criteria for a poor prognosis.
Conclusion
LV remains a rare cause of gastric perforation. This is a surgical emergency requiring partial or total gastric resection depending on the extent of the necrosis. Improved prognosis depends on early diagnosis and treatment of chronic and sub-acute forms.
References
- Carter R, Brewer LA, Hinshaw DB (1980) Acute gastric volvulus. A study of 25 cases. Am J Surg 1980 140: 90-106.
- Menguy R (1995) Le traitement chirurgical des hernies hiatales par roulement avec volvulus intrathoracique de la totalite´ de l’estomac. Chirurgie 120: 439-443.
- Alamowitch B, Christophe M, Bourbon M, Porcheron J, Balique JG (1999) Hernie hiatale paraoesophagienne avec volvulus gastrique aigue¨. Gastroenterol Clin Biol 23: 271-274.
- Bedioui H, Bensafta Z (2008) Volvulus gastrique: diagnostic et prise en charge thérapeutique. Presse Med. 37: e67-e76.
- Hillemand P, Bernard HJ, Villard J (1955) A propos des volvulus gastriques.Sem HopParis 31: 2890-2899.
- Grignon B, Sebbag H, Reibel N, Zhu X, Grosdidier G, et al. (2004) Diagnostic tomodensitométrique d’un volvulus. 85: 1070-1073.
- Godshall D, Mossallam U, Rosenbaum R (1999) Gastric volvulus: Case report and review of literature. J Emerg Med 17:837-840.
- Cloyd DW (1994) Laparoscopic repair of incarcerated paraoesophageal hernia. Surg Endosc 8: 893-897.
- Cameron AE, Howard ER (1987) Gastric volvulus in childhood. J Pediatr Surg 22: 944-947.
- Benoit L, Goudet P, Cougard P (1997) Acute intraabdominal gastric volvulus in adults. Defect of dorsal mesogastrium fusion. Ann Chir 51: 379-381.
- Aliye U, Simon C, Kao D, Kathleen D, Lawrence J (1998) Gastric volvulus and wandering spleen. Am J Gastroenterol 93: 1146-1148.
- Qazi A, Awadallah S (2004) Wandering spleen: a rare cause of mesenteroaxial gastric volvulus. Pediatr Surg Int 20: 878-880.
- Larricq J (1998) Pathologie gastrique rare. EMC Gastroente´ rologie 9-031-B-10: 1-3.
- Shivanand G, Seema S, Srivastava DN, Pande GK, Sahni P, et al. (2003) Gastric volvulus Acute and chronic presentation. Clinical Imaging 27: 265-268.
- Chafke N, Wihlm JM, Massard G, Morand G, Witz JP (1988) La hernie retro-costo-xiphoïdienne. Proble` mes de diagnostic et de traitement. A propos de huit observations. Ann Chir 42: 467-473.
- Honna T, Kamii Y, Tsuchida Y (1990) Idiopathic gastric volvulus in infancy and chilhood. J Pediatr Surg 25: 707-710.
- Arimont JM, Ramoisiaux L, Majerus B (1998) Cure laparoscopique d’une hernie rétro-costoxyphoidienne compliquée d’une occlusion par volvulus gastrique intrathoracique. Ann Chir 52: 660-664.
- Smith J, Ghani A (1995) Morgani hernia:incidental repair during laparoscopic cholecystectomy. J Laparoendosc Surg 5: 123-125.
- Uc A, Kao SC, Sanders KD, Lawrence J (1998) Gastric volvulus and wandering spleen. Am J Gastroenterol 93: 1146-1148.
- Gonzalez JJ, Alvarez PJA (1991) Volvulus gastrique. EMC Gastroenterologie 9-031-B-12.
- Bedioui H, Bensafta Z (2008) Volvulus gastrique : diagnostic et prise en charge thérapeutique. Presse Med 37: e67–e76.
- Rantomalala HY, Rajaonarivony T, Rakototiana AF, Rakotoarisoa AJ, Ramarosandratana JL, Razakatiana L, et al. (2005) Un cas de volvulus aigu de l?estomac chez l?enfant . Archives de pédiatrie 12: 1726-28.
- Herinirina SAE, Rasataharifetra H, Rasamoelina Rakotoarijaona AH, Ratsivalaka R (2010) Un cas de volvulus gastrique aigu de l’adulte au Centre Hospitalier Universitaire de Toamasina. Revue Tropicale de Chirurgie 4: 22- 23.
- Miller DL, Pasquale MD, Seneca RP, Hodin E (1991) Gastric volvulus in the pediatric population. Arch Surg 9: 1146-1149.
- Kuwano H, Hachizume M, Sumiyoshi K, Sugimachi K, Haraguchi Y (1998) Laparoscopic repair of a paraoesophageal hiatal hernia with gastric volvulus. Hepatogastroenterology 45: 303-306.
- Alamowitch B, Boubon M, Porcheron J, Pyneeandee S, Balique JG (1995) Volvulus gastrique aigue¨ sur hernie hiatale revelee par une lithiase chole´ docienne. J Chir (Paris) 132: 454-458.
- Christophe M, Rat P, Sala JJ, Dia A, Favre JP (1989) Le volvulus intrathoracique de l’estomac dans les hernies hiatales. Sem Hop Paris 65: 2583-2587.
- Leblanc I, Scotte M, Michot F, Teniere P (1991) Incarce´ ration gastrique sur hernies hiatales para-oesophagiennes et par glissement.Ann Chir 1991;45:42-5.
- Haas O, Rat P, Christophe M, Friedman S, Favre JP (1990) Surgical results of intrathoracic gastric volvulus complicating hiatal hernia.Br J Surg 77: 1379-1381.
- Harriss DR, Graham TR, Galea M, Salama FD (1992) Paraoesophageal hernia: when to operate? JR Coll Surg Edinb 37: 97-98.