Publication Information
ISSN: 2641-693X
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2018
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Awareness, Knowledge and Critical Resuscitation Skills among Health Care Professionals of a Tertiary Health Care Facility
Arslan MASOOD*, Noor DASTGIR, Zubair AKRAM, Ayesha HANIF, Tariq Iqtidar Sadiq SYED, Usman SADIQ
Department of Cardiology, Allama Iqbal Medical College, Jinnah Hospital, Lahore, Pakistan
Received Date: December 29, 2018; Accepted Date: January 4, 2019; Published Date: January 15, 2019
*Corresponding author: Arslan MASOOD, Department of Cardiology, Allama Iqbal Medical College, Jinnah Hospital, Lahore, House # 229, Tariq Block, New Gardentown, Lahore, Pakistan. Tel: +92 3214353909; Email: dr_arslanmasood@hotmail.com
Citation: Masood A, Dastgir N, Akram Z, Hanif A, Syed TIS, Sadiq U (2019) Awareness, Knowledge and Critical Resuscitation Skills among Health Care Professionals of a Tertiary Health Care Facility. Inte Jr Cardiac Scie and Res: IJCSAR-108.
Abstract
Background:
Health care professionals of South-Asia and other developing countries lack basic life support / cardiopulmonary resuscitation education and training is often deficient in these regions. We conducted this study to assess the knowledge and status of training and certifications across health care professionals regarding CPR/BLS recommendations at a tertiary care hospital facility and its affiliated medical school.
Methods:
The survey included 320health care professionals including doctors and medical students. Questionnaire based data was collected to assess the general awareness regarding BLS and CPR guidelines, institutes offering BLS/CPR training, status of previous BLS/CPR training and involvement in real time BLS/CPR activities. A separate segment of the questionnaire was assessed “critical BLS and CPR knowledge” and a “critical knowledge score” was derived from aggregate of correctly answered critical BLS and CPR knowledge questions.
Results:
The study included 46.6% male and 53.4% female health care professionals.47.2% (151) of them had attended at least some sort of BLS or CPR training course or workshop in the past and 46.1% (158) had provided BLS or CPR at least once in their careers. Mean critical knowledge score for BLS and CPR skills was 4.79 ± 2.7(95% CI 4.5 – 5.1). Qualified physicians scored better than the medical students 5.7 ± 2.6 vs 2.8±1.7 (p < 0.001, 95% CI 2.3 – 3.4). Health care professionals with previous participation in BLS / CPR training courses scored better compared to those without such training 5.9 ± 2.4 vs 3.8 ± 2.6 (p < 0.001, 95% CI 1.5 – 2.6).
Conclusions:
Data from this South-Asian tertiary care center shows that the knowledge and skills of health care professionals regarding BLS/CPR skills is generally poor. Health care professionals with participation in previous training courses show relatively better knowledge, however in absolute terms, it is still remarkably lower than expected and quite inadequate.
Keywords: Basic Cardiac Life Support; Cardio Pulmonary Resuscitation; Sudden Cardiac Arrest; Sudden Death
Background
Cardiopulmonary arrest is generally associated with low survival rates depending upon delays in initiation of resuscitative efforts, cardiopulmonary resuscitation (CPR) techniques and time to defibrillation [1,2]. For every minute without CPR, survival decreases by almost 10%, in a patient of cardiac arrest due to ventricular fibrillation [3]. Chances of survival from sudden cardiac arrest can be increased two to three folds with early CPR [4]. Techniques of basic life support (BLS) have been seen through the early 17th centuries; over time they have developed into proper protocols. CPR is perhaps one of the difficult skills to master but its importance cannot be measured or valued enough. It is mandatory for health care professional (HCPs) to acquire appropriate resuscitative knowledge and skills, however, such skills are poorly retained and knowledge of HCPs is often outdated due to insufficient refresher programs to keep up with guideline updates [5]. BLS training courses are helpful in improving knowledge and skills of CPR [6]. Challenges faced during the acquisition of adequate CPR skills not only include the difficulty for the first-time learner but also with retention of the acquired knowledge [7,8].
Healthcare systems vary across the globe in terms of legislation and regulations for CPR training and certification requirements of HCPs before the start of their careers and refresher programs thereafter. In contrast to developed western healthcare systems, South-Asia and other developing countries lack strict regulations in this regard, therefore, CPR/BLS education and training is often deficient in these regions. Similarly, there is lack of refresher courses to update the knowledge and improve upon former techniques according to updated and revised guidelines. We conducted this study to assess the awareness, knowledge and status of training and certifications across doctors and medical students regarding CPR/BLS recommendations at a tertiary care hospital facility and its affiliated medical school. The findings of this study will help to strengthen the justification to enhance efforts for improvement of training programs as well as refresher courses and amend medical licensing regulations by identifying the gaps of current training, knowledge and skills among HCPs.
Methods
The cross-sectional questionnaire-based survey included 320 HCPs including undergraduate medical school students, house physicians (within first year of their clinical practice after medical graduation), post-graduate medical residents and medical consultant physicians. Study participants were recruited by consecutive sampling from various departments of a tertiary care hospital and its affiliated medical school.
A pre-validated questionnaire was used to assess the knowledge and attitude towards BLS and CPR skills. The questionnaire was designed to assess general awareness regarding BLS and CPR guidelines, institutes offering BLS/CPR training, status of previous BLS/CPR training and real time involvement in such activities. A separate segment of the questionnaire assessed “critical BLS and CPR knowledge” (Table 1). The participants had to select the best out of closely matched choices. 1. What is the first recommended step to be followed for non-responsive victims? 2. What is the current recommended sequence of “Airway”, “Breathing” and “Circulation” in terms of preference? 3. What is the maximum permitted time for pulse-check? 4. What is the recommended site for chest compressions? 5. What is minimum recommended depth of chest compressions for effective adult CPR? 6. What is the minimum recommended rate of chest compressions for effective adult CPR? 7. What is recommended compression-ventilation ratio for adult CPR? 8. What is recommended rate of rescue breaths with advanced airway in place during CPR for adults? 9. Which is the appropriate device to be used in BLS sequence other than airways assistances? 10. What is the most commonly encountered shock able arrhythmia in collapsed victims? 11. What is the recommended appropriate next step after defibrillation?
Sr.No
BLS and CPR Critical Skills Knowledge Questions
Matching Answers (Correct answers in Bold)
a) Call for help/ activation of emergency response system
b) Start chest compressions
c) Give rescue breaths
d) Check for carotid pulse and assess breathing
a) Airway- Breathing-Circulation “A-B-C”
b) Breathing-Circulation- Airway “B-C-A”
c) Circulation-Airway-Breathing “C-A-B”
d) Airway-Circulation-Breathing “A-C-B”
a) 2 seconds
b) 5 seconds
c) 10 seconds
d) 30 seconds
a) Xiphisternum
b) Mid-sternum, at the level of plane traversing nipples.
c) Left side of sternum
d) Upper end of sternum
a) 1 inch or 2.5 cm
b) 2 inches or 5 cm
c) 5 inches or cm
d) Half the anteroposterior thoracic diameter
a) 50/min
b) 60/min
c) 100/min
d) 120/min
a) 5:2 compressions-breaths ratio
b) 10:2 compressions-breaths ratio
c) 15:2 compressions-breaths ratio
d) 30:2 compressions-breaths ratio
a) 4 to 6 breaths per minute
b) 8 to 10 breaths per minute
c) 14 to 16 breaths per minute
d) 18 to 20 breaths per minute
a) Automated external defibrillator
b) Ryle’s tube
c) Central venous line
d) End tracheal tube
a) Completer AV block
b) Ventricular fibrillation / pulseless ventricular tachycardia.
c) Atrial fibrillation
d) Sinus tachycardia
a) Resume chest compressions
b) Assess the rhythm
c) Repeat defibrillation
d) Check for pulse
The data was computed and analyzed by software Statistical Package for Social Sciences (SPSS Version 23, IBM). A “Critical Knowledge Score” was derived from aggregate of correctly answered critical BLS and CPR.
knowledge questions, all carrying equal marks. The scores were calculated based on rate of correct answers out of total eleven critical knowledge questions, ignoring the wrong answers without negative marking. Individual scores for all HCP categories were calculated as means ± SD and 95% CIs. HCPs categories were segregated into two groups; ‘qualified physician’ (composite of consultants, postgraduate residents and house physicians) and medical students. The two groups were compared for their respective critical BLS and CPR knowledge score means by independent samples t-test. A similar comparison of mean scores was carried out between two groups based on participation in previous BLS/ CPR training courses to assess the potential confounding impact of such training courses on critical skills knowledge.
The score was further stratified into three groups with ≥ 7score considered as adequate critical knowledge, while ≤ 4 score as poor critical knowledge. Frequencies and percentages of adequate and poor knowledge statuses were compared among HCP categories by Pearson’s chi-square.
Results
The study included 46.6% male and 53.4% female HCPs;82 (25.6%) post graduate residents, 122 (38.1%) house physicians, 17 (5.3%) consultant physicians and 99 (30.9%) medical students. Regarding general awareness of BLS and CPR, 16.2% (52) healthcare providers had not ever heard of the term “BLS”, 13.1% (42) did not know what “BLS” abbreviation stood for and 3.7% (12) did not know what “CPR” abbreviation stood for. Awareness regarding guidelines and training in BLS and CPR skills was also poor; 77.2% (247) healthcare providers did not know national facilities that offered training in BLS and 40% (128) did not know of any international BLS and CPR guidelines issuing organizations. 47.2% (151) health care providers had attended at least some sort of BLS or CPR training course or workshop in the past and 44.4% (142) had provided BLS or CPR at least once in their careers.
Mean critical knowledge score for BLS and CPR skills was 4.79± 2.7(95% CI 4.5 – 5.1) (Table 2). ‘Qualified physicians’ scored better than medical students (p < 0.001, 95% CI 2.3 – 3.4) (Figure 1).
N
Mean ± SD (95% CI of mean)
Postgraduate Residents
82
5.56 ± 2.9 (4.9 – 6.2)
House physicians
122
5.84 ± 2.3 (5.4 – 6.3)
Consultants
17
4.82 ± 3.2 (3.2 – 6.5)
Medical students
99
2.86 ± 1.7 (2.5 – 3.2)
All HCPs
320
4.79 ± 2.7 (4.5 – 5.1)
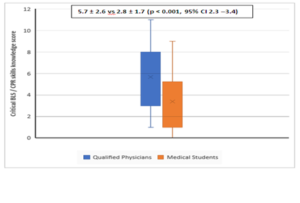
Figure 1: Comparison of critical BLS / CPR skills knowledge score between qualified physicians and other HCPs (independent samples t-test). HCPs with previous participation in BLS / CPR training courses scored better compared to those without such training (p < 0.001, 95% CI 1.5 – 2.6) (Figure-2).

Figure 2: Impact of previous training course participation on critical BLS / CPR skills knowledge score (independent samples t-test).
Only 28.4% (91) HCPs scored adequate (37.8% of postgraduate residents, 40.1% of house physicians, 35.3% of consultants and 4% of medical students) and 39.7% (127) HCPs scored poor (30.5% of postgraduate residents, 14.8% of house physicians, 47.1% of consultants and 76.8% of medical students) (Figure 3).
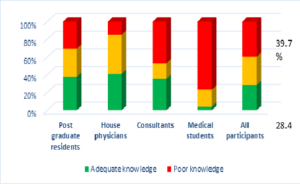
Figure 3: Fractions of HCPs with adequate knowledge and poor knowledge of critical BLS and CPR skills (Pearson’s chi-square).
Frequencies and percentages of correct answers to the BLS technical knowledge testing questions by various health care provider categories are tabulated (Table 3). (N= 122) (N= 343)
Sr.
Critical Knowledge Testing Questions
Post-graduate Residents (N= 82)
House Physicians
Consultants (N= 17)
Medical Students (N= 99)
TOTAL
1
First step for non-responders
30 (36.6%)
60 (49.1%)
1 (5.9%)
10 (10.1%)
101 (31.6%)
2
Correct CAB sequence
46 (56.1%)
54 (44.3%)
9 (52.9%)
29 (29.3%)
138 (43.1%)
3
Pulse check duration
28 (34.1%)
57 (46.7%)
7 (41.1%)
18 (18.2%)
110 (34.4%)
4
Chest compression location
35 (42.7%)
56 (45.9%)
11 (64.7%)
38 (38.4%)
140 (43.7%)
5
Chest compression depth
48 (58.5%)
67 (54.9%)
10 (58.8%)
51 (51.5%)
176 (55%)
6
Minimum compression rate
51 (62.3%)
74 (60.6%)
7 (41.2%)
12 (12.1%)
144 (45%)
7
Compression ventilation ratio
60 (73.1%)
109 (89.3%)
9 (52.9%)
17 (17.2%)
195 (60.9%)
8
Ventilation rate with advanced airway
31 (37.8%)
42 (34.4%)
9 (52.9%)
32 (32.3%)
114 (35.6%)
9
Appropriate BLS device
55 (67.1%)
92 (75.4%)
12 (70.6%)
62 (62.6%)
221 (69.1%)
10
Shock able rhythm identification
36 (43.9%)
58 (47.5%)
4 (23.5%)
4 (4%)
102 (31.9%)
11
Next step after shock
28 (34.1%)
43 (35.2%)
4 (23.5%)
3 (3%)
78 (24.4%)
Discussion
Deficiencies in in-hospital and out-of-hospital CPR qualities have been highlighted in several publications.(9)Our study showed poor general awareness for BLS and CPR, poor knowledge of guidelines, lack of awareness about training institutes and only 47.2% of study participants had previous BLS or CPR training. A small number of HCPs in our study (13.1%) were not even familiar with the term “BLS”. Chandrasekaran et al reported even lesser familiarity with the term where 31% of the responders did not know the abbreviation of BLS as “Basic Life Support” [10].
Undergraduate medical students were least knowledgeable among all HCPs in our study, emphasizing the dire need to start compulsory BLS/CPR training courses for such individuals towards the start of their medical careers. Medical curricula are largely lacking in BLS education and training [11,12]. The General Medical Council of UK recommends house officers to be BLS trained before their first posting and to get advanced life support training during the first year [13]. Likewise, the Royal College of Physicians recommended teaching advanced life support to undergraduates and making pre-registration house officers capable of instituting such skills [14]. There has been evidence from earlier studies showing school children, as young as nine-years, to have adequate cognition for performing CPR after specific training [15,16].
In our study, HCPs performed poorly with respect to their knowledge for BLS/CPR skills. Overall, only 28.4% (91) HCPs possessed adequate knowledge by correctly answering at least 7 questions pertaining to critical knowledge assessment. Among remaining, 39.7% (127) HCPs even performed poorly by correctly answering only four or lesser questions. The mean scores were very low for all HCP categories, exposing their lack of knowledge regarding these life-saving scientific actions and maneuvers. An Indian study concluded that awareness of BLS among students, doctors and nurses of medical, dental, homeopathy and nursing colleges was very poor [17].
American Heart Association identified complexity of CPR steps and their poor retention after training completion as major factors influencing long term knowledge and skills of HCPs exposed to such training courses [18]. Previous experience in real life resuscitation activities, however, has been demonstrated to impact retention of knowledge [19]. The composite group of qualified physicians in our study showed better knowledge compared to medical students statistically, however in absolute terms, the scores by the earlier group were remarkably lower than expected and quite inadequate. Although, participation in previous BLS or CPR training workshops or courses was associated with statistically better scores compared to those lacking such exposures or experiences, the knowledge was still clinically inadequate. This logically supports the fact that training courses and workshops do help in improving knowledge and skills, but there need to be timely refreshers, renewals or periodic assessments in order to maintain minimum standards, impact long term cognitive learning and develop correct emergency resuscitative reflexes among HCPs.
Further multi-center randomized studies on the subject are required to strengthen these observations and highlight the dire need to improve standards of BLS and resuscitation skills among HCPs. Moreover, such studies should also include demonstration of practical skills by HCPs.
Conclusion
Data from this South-Asian tertiary care center shows that the knowledge and skills of HCPs regarding BLS/CPR skills is generally poor. HCPs with participation in previous training courses show relatively better knowledge, however in absolute terms, it is still remarkably lower than expected and quite inadequate.
List of Abbreviations
BLS : Basic life support
CPR : Cardiopulmonary resuscitation
HCPs : Health care professionals
SPSS : Statistical package for social sciences
Declarations
- Ethics approval and consent to participate: The research project was approved by “Ethical Review Board, Allama IQBAL Medical College/ Jinnah Hospital Lahore”.
- Consent for publication: “Not applicable”
- Availability of data and material: The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
- Competing interests: “The authors declare that they have no competing interests”
- Funding: Funding related to data collection was borne by the corresponding author.
Authors’ Contributions
Arslan MASOOD – Designing the study, Data analysis and interpretation
Noor DASTGIR – Literature search, Manuscript writing
Zubair AKRAM – Conception, Study designing, Critical revision
Ayesha HANIF – Data collection and compilation, Literature search
Tariq Iqtidar Sadiq SYED – Data collection and compilation
Usman SADIQ – Data collection and compilation
Acknowledgements: “Not applicable”
References
- Wik L, Steen PA, Bircher NG (1994) Quality of bystander cardiopulmonary resuscitation influences outcome after prehospital cardiac arrest. Resuscitation 28: 195-203.
- Gwinnutt C, Columb M, Harris R (2000) Outcome after cardiac arrest in adults in UK hospitals: effect of the 1997 guidelines. Resuscitation 47: 125-135.
- MacDonald RD, Mottlay JL, Weinstein C (2002) Impact of prompt defibrillation on cardiac arrest at a major international airport. Prehosp Emerg Care 6: 1-5.
- Adult basic life support (2005) American heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 112: IV1 -203.
- Federico S, Luciano S, Erga L (2006) Retention of CPR performance in an aesthetists. Resuscitation 68: 101-108.
- Chaudhary A, Parikh H, Dave V (2011) Current scenario: Knowledge of basic life support in medical college. Natl J Med Res 1: 80-82.
- Christenson J, Nafziger S, Compton S, Vijayaraghavan K, Slater B, et al. (2007) The effect of time on CPR and automated external defibrillator skills in the Public Access Defibrillation Trial. Resuscitation 74: 52-62.
- Shrestha R, Batajoo KH, Piryani RM, Sharma MW (2012) Basic life support: knowledge and attitude of medical/paramedical professionals. World J Emerg Med 3: 141-145.
- Shrestha R, Batajoo K, Piryani R, Sharma MW (2012) Basic life support: knowledge and attitude of medical/paramedical professionals. World J Emerg Med 3: 141-145.
- Chandrasekaran S, Kumar S, Bhat SA, Saravanakumar, Shabbir PM, et al. (2010) Awareness of basic life support among medical, dental, nursing students and doctors. Indian J Anaesth 54: 121-126.
- Zaheer H, Haque Z (2009) Awareness about BLS (CPR) among medical students: status and requirements. J Pak Med Assoc 59: 57-59.
- Casey WF (1984) Cardiopulmonary resuscitation: a survey among junior hospital doctors. J R Soc Med 77: 921-924.
- Philips PS, Nolan JP (2001) Training in basic and advanced life support in UK medical schools: questionnaire survey. BMJ 323: 22-23.
- Royal College of Physicians of London (1987) Resuscitation from cardiopulmonary arrest. J R Coll Physicians Lond 21: 175-182.
- Kelley J, Richman P, Ewy G, Clark L, Bulloch B, et al. (2006) Eighth grade students become proficient at CPR and use of an AED following a condensed training program. Resuscitation 71: 229-236.
- Fleischhackl R, Nuernberger A, Sterz F, Schoenberg C, Urso T, et al. (2009) School children sufficiently apply life supporting first aid: a prospective investigation. Crit Care 13: R127.
- Chandrasekaran S, Kumar S, Bhat SA, Saravanakumar, Shabbir PM, et al. (2010) Awareness of basic life support among medical, dental, nursing students and doctors. Indian J Anaesth 54: 121-126.
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, et al. (2010) Heart disease and stroke statistics-2010 update: a report from the American Heart Association. Circulation 121: 948-954.
- Elif AA, Zeynep K (2003) Knowledge of basic life support: a pilot study of the Turkish population by Baskent University in Ankara. Resuscitation 58: 187-192.
