Publication Information
ISSN 2691-8803
Frequency: Continuous
Format: PDF and HTML
Versions: Online (Open Access)
Year first Published: 2019
Language: English
| Journal Menu |
| Editorial Board |
| Reviewer Board |
| Articles |
| Open Access |
| Special Issue Proposals |
| Guidelines for Authors |
| Guidelines for Editors |
| Guidelines for Reviewers |
| Membership |
| Fee and Guidelines |
 |
Mortality at the Medical Emergency Department in a University Teaching Hospital in Ouagadougou (Burkina Faso)
Eric Nagaonlé Somé1*, Djingri Labodi Lompo2, Abdoul Sawadogo3, Roger Sombié4, Maxime Drabo1
1Département biomédical et santé publique, Institut de Recherche en Sciences de la Santé (IRSS) Ouagadougou, Burkina Faso
2Unité de Formation et de Recherche en Sciences de la Santé, département de médecine et Spécialités médicales, section neurologie, Université Joseph Ki-Zerbo de Ouagadougou ; Burkina Faso
3 ONG Terre des Hommes, Ouagadougou, Burkina Faso
4 Unité de Formation et de Recherche en Sciences de la Santé, département de gastro-entérologie, Université Joseph Ki-Zerbo de Ouagadougou, Burkina Faso
Received Date: November 30, 2021; Accepted Date: February 7, 2022; Published Date: February 14, 2022;
*Corresponding author: Eric Nagaonlé Somé, Département biomédical et santé publique, Institut de Recherche en Sciences de la Santé (IRSS) Ouagadougou, 10 BP 250 Ouagadougou, 10; Burkina Faso, Tel : +226 70 75 13 33. Email: eric.some@gmail.com
Citation: Somé EN, Lompo DL, Sawadogo A, Sombie R, Drabo M (2022) Mortality at the medical emergency department in a university teaching hospital in Ouagadougou (Burkina Faso). Adv Pub Health Com Trop Med. APCTM-136.
DOI: 10.37722/AOASM.2022011
Abstract
Introduction
Our objective was to study the mortality of people aged 60 years and over at the medical emergency unit of the Yalgado Ouédraogo University Teaching Hospital.
Methods
It was a cross-sectional, descriptive study with a retrospective data collection from January 2010 to December 2017. The study population consisted in people of both genders aged 60 years or over and having stayed at the medical emergency department during the study period.
Results
The mortality rate was 30.2%. The mean age among deceased patients was 62 years. The age group of 60 -70 years was the most represented with 60% of the total mortality. With respect to the occupation, housewives and farmers were the most represented with 38.4% and 27.9% of those who passed away, respectively; 86% of them had a history of cardio-vascular disease. Cardiovascular attacks, malaria and respiratory diseases were the main diagnostic hypotheses at entry with 23.22%, 12.99% and 11.67% of cases respectively. Over the eight years, the peaks of deaths were recorded in the months of January, April, October and November. The lowest rates were in March.
Conclusion
Dying between the ages of 60 and 70 is still quite early compared to more developed countries. Non-sophisticated measures such as educating the elderly to permanent hydration, especially during periods of extreme heat, could reduce these gloomy statistics.
Keywords: Burkina Faso; Elderly; Emergency Unit; Mortality Rate; Sub Saharan Africa
Introduction
Many developed countries have a large population of older people with around 20% of the total population aged 60 years and over. In resource-limited settings, less than 10% of the population is 60 years or older. Unlike developed countries where the transition to aging has gradually taken hold over at least a century, developing countries will reach the same level of aging in the span of about half a century (1). The growing number of older people and the inherent complexity of the management of their health have resulted in an increased demand on the health care system (2, 3), including emergency inpatient services, outpatient care, home visits and long-term care including palliative care (4). It has been established in developed countries that older people use health services up to 4 times more (5) and that they are three times more likely to be hospitalized than younger people (6). Hospitalization of the elderly is in itself a challenge. In fact, for the same diagnosis, they are more likely to experience complications and stay in hospital longer than young people (7). Also, higher mortality has been reported among hospitalized elderly people, ranging from 5% during hospital stay to 20-30% in the year following hospital discharge (6).
In sub-Saharan Africa, few studies have dealt with hospital mortality in the elderly. In these studies, hospital mortality rates ranged from 15.1% in South Africa (8), to 22% in Nigeria (9). In Togo, all-cause mortality in elderly was 17.2%. About 93.7% of elderly deaths occur in hospital.
In Burkina Faso, the proportion of people aged 65 or over remained 3.4% between 2015 and 2019 (8). However, aging takes place in a context of a weak and under-equipped health system which struggles to bear the burden of hospitalizations for the elderly (10). The level of general mortality still remains high although there was a decrease between 1996, 2015 and 2020 with crude death rates of 14.8 ‰, 11.8 ‰ (8, 11) and 8.7 %, respectively. Life expectancy at birth increased from 59 years in 2010 to 62 years in 2015 (8) and 61.8 years in 2018 (https://www.indexmundi.com/fr/burkina_faso/esperance_de_vie_a_la_naissance.html). The two factors (mortality and life expectancy) combined with declining fertility, resulted in an aging of the population, which is a worldwide phenomenon. Our objective was to study the mortality of people aged 60 years and over in the medical emergency unit of the Yalgado Ouédraogo University Teaching Hospital.
Population and Methods
It was a cross-sectional, descriptive study with a retrospective data collection from January 2010 to December 2017 in the medical emergency department of the Yalgado Ouédraogo University Teaching Hospital. The study population consisted of people of both genders aged 60 years or over and having stayed in the medical emergency department during the study period. Patients who died by accidents and those not residing in the city of Ouagadougou were excluded. Data were collected from the medical records of the patients hospitalized in the department. The numbers of deaths per month were aggregated into years. We run descriptive statistics with means (continuous variables) and proportion (categorical variables) calculation. Data were analyzed using the statistical program for social sciences (SPSS) version 16.0 software.
Results
A total of 1208 cases were included; Male gender represented 59.76%. Over 80% of the women were housewives, and 52.04% of the men were farmers.
Overall, 365 people died. The mortality rate was 30.2%. The mean age was 62 years. The age group of 60 -70 years was the most represented with 60% of the total mortality. The age ranged from 60 to 109 years. With respect to the occupation, housewives and farmers were the most represented with 38.4% and 27.9% of those who passed away, respectively; 86% of them had a history of cardio-vascular diseases. Among the reasons that prompted the medical visits from the participants, poor condition, general, respiratory and neurological symptoms represented 18.73%, 17.90%, 17.90% and 16.77%, respectively. Cardiovascular attacks, malaria and respiratory diseases were the main diagnostic hypotheses at entry with 23.22%, 12.99% and 11.67% of cases respectively (Table 1). Over the eight years, the peaks of deaths of people aged 60 and over were recorded in the months of January, April, October and November. The lowest rates were in March (Figure 1).
Characteristics
Number (N=365)
Percentage
Age groups
60 – 70
219
60
71 – 80
110
30
>80
36
10
Occupation
Housewives
140
38,4
Farmers
102
27,9
Retired
48
13,1
Traders
28
7,8
Others
47
12,9
Medical history
Cardio-vascular disease
314
86
Kidney disease
36
10
Others
15
4
Reasons of medical visits
Poor condition
181
18,73
Respiratory symptoms
173
17,90
General symptoms
173
17,90
Neurologic symptoms
162
16,77
Cardio-vascular symptoms
126
13,04
Other reasons
151
15,63
Temperature at entry
Hyperthermia
223
61
Hypothermia
88
24
Normal temperature
55
15
Diagnostic hypothesis
Cardio-vascular attacks
177
23,22
Malaria
99
12,99
Respiratory disease
89
11,67
Other heart disease
64
8,39
Kidney disease
64
8,39
Neurologic disease
53
6,95
Digestive disease
49
6,43
Other
167
21,91
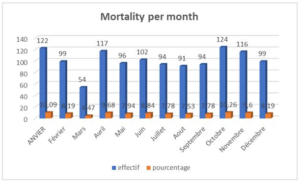
Figure 1: Distribution of the mortality per month.
Discussion
Mortality was higher in men (59.76%) than in women. Similar results were obtained in a previous study implemented in a semi-rural area in Burkina Faso in 2010 and the mortality rate was 56.09% among men. A report from the Burkina Faso health ministry also recognized in 2015 that women lived longer than men in the country (1). Most of the deceased men were farmers and the deceased women were housewives. These statistics seems aligned with the context of Burkina Faso which is a country where the main occupation is farming. The mean age of deceased patients was 62 years, which is comparable to the life expectancy (61.8 years) in Burkina Faso according to a World Bank study in 2018 (2).
Peak mortality was observed in January, April, October and November. The deaths observed in January could be explained by the harmattan or dried season with a lots of dusty winds, which would result in a proliferation of infectious germs. Deaths in April could be due to the high temperature and heatwaves. With age, the natural regulation system which allow controlling the body temperature is no more working properly. The direct consequence would be disturbances in the internal body temperature. This was also found by Oudin A. Et al in 2015; The responses to the heat stress are altered in older people, and these individuals are more vulnerable because of increases in red blood cell and platelet count and cholesterol level, resulting in more heat-induced blood viscosity.
These abnormalities could lead to cerebral thromboses (3). Dehydration is another common cause of hyperthermia leading to death in elderly. It also slows down the rate of sweating, according to a joint report by the World Health Organization and the World Meteorology Organization in 2015 (4). Since the elderly have impaired thermoregulation, and are more prone to chronic diseases, heat stress triggers these diseases which will sometimes lead to death. Different studies implemented in developed countries also identified the elderly groups as the most vulnerable to heat, both in terms of mortality and morbidity (4-6). The months of October and November correspond to the months of most frequent medical visits, because it is during this period that vector-borne diseases such as malaria and dengue are rife. These diseases claim many victims every year. These months correspond to the immediate post-rainy period which is the period that generates several vector nests.
All participants had a medical history. This seems normal because aging is a risk factor for many diseases. A cardio-vascular history was the most common one and the cardiovascular failure was the leading cause of death during heat waves. In general, any chronic condition should be considered as a potential risk factor for morbidity and mortality in the elderly (4, 12).
The deterioration of the patient’s general health status (18.7%) was the main reason for medical visit, followed by dyspnea, general and cardiac symptoms. Several diagnostic hypotheses were enumerated after the medical visits. Cardiovascular attacks were the most diagnosed pathology with a percentage of 23.22%, while malaria was evoked in only 12.99% and digestive dysfunctions 6.43% of the cases. Usually, patients only go to hospital when their general health condition has completely worsen. The reason is mainly the threat of the expenses associated to medical visits and this threat leads to self-medication including traditional medicines administration. Malaria cases are probably under-estimated, knowing that the deterioration of the general health status and the other mentioned symptoms could also be related to an ongoing malaria disease. According to the Burkina Faso ministry of health, malaria is the first reason for medical visit in Burkina. After the malaria cases, follow the respiratory diseases in frequency. These results observed among our deceased participants are similar to the ones obtained in the general population of the elderly. In terms of diagnosis, overall cardiac pathologies accounted for about 30% of all diagnosed pathologies. Several other studies have found high prevalence of cardiovascular events that can lead to mortality in the elderly (1, 2). Jie Ban et al (3) associated increased mortality with acute myocardial infarction, coronary heart disease and stroke (2.4% to 14.3%); these different pathologies are all due to a high environmental temperature.
Study limitations
This mortality study was limited to the medical emergency department, while there are several other emergency departments within the same hospital. The results are therefore incomplete and cannot describe the whole reality of the elderly mortality in the main tertiary hospital in Ouagadougou. In the medical emergency department, there was a large number of missing patients’ records. Another limitation is that the analyzed records, most often, did not help us with an accurate diagnoses.
Conclusion
Dying between the ages of 60 and 70 is still quite early compared to more developed countries. Simple, non-sophisticated measures such as educating the elderly to permanent hydration, especially during periods of extreme heat, could reduce these gloomy statistics. Prospective observational as well as experimental studies are necessary to better understand the mortality risk factors as well as the potential responses adapted to the context of Burkina Faso.
Declarations
Conflict of interest/competing interest: The authors declare no conflicting or competing interest.
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’ contributions
ENS: Conceptualization; Methodology; Supervision; Project administration; Data Curation; Writing – Original Draft; Writing – Review & Editing
DLL: Conceptualization; Methodology; Writing – Review & Editing
AS: Writing – Review & Editing
MKD: Methodology; Writing – Review & Editing
RS: Conceptualization; Methodology Writing – Review & Editing
Acknowledgement
We are much grateful to the staff of the gastro-enterology department who contributed greatly to and facilitated the data collection. We want also to thank the administration of the university teaching hospital Yalgado Ouedraogo who provided all permission to make possible the data collection.
References
- Sajoux M, Nowik L (2012) Conclusion. De la transition au vieillissement démographique. Nouvelles réalités, nouveaux enjeux. Les Cahiers d’emam. 21:113-5.
- Han J, Liu S, Zhang J, Zhou L, Fang Q et al. (2017) The impact of temperature extremes on mortality: a time-series study in Jinan, China. BMJ Open, 7:e014741.
- Oudin Astrom D, Schifano P, Asta F, Lallo A, Michelozzi P et al. (2015) The effect of heat waves on mortality in susceptible groups : a cohort study of a mediterranean and a northern European City. Environmental health : a global access science source.14:30.
- Ban J, Xu D, He MZ, Sun Q, Chen C et al. (2017) The effect of high temperature on cause-specific mortality: A multi-county analysis in China. Environ Int. 106:19-26.
- Jourdain A, Gardin G, Frinault T (2004) Épisode caniculaire et personnes âgées Éléments localisés de diagnostic, d’alerte et de plan d’urgence Synthèse des études réalisées dans les régions Île-de-France, Centre, Bourgogne, Auvergne, Haute-Normandie et Franche-Comté [document de travail]. Direction de la recherche, des études, de l’évaluation et des statistiques (DREES), Ministère de l’emploi, du travail et de la cohésion sociale, Ministère de la santé et de la protection sociale, 43:66.
- Cadot E, Spira A (2006) Canicule et surmortalité à Paris en août 2003. Espace populations sociétés, 239-49.
- Medina-Ramon M, Zanobetti A, Cavanagh DP, Schwartz J (2006) Extreme temperatures and mortality: assessing effect modification by personal characteristics and specific cause of death in a multi-city case-only analysis. Environ Health Perspect. 114:1331-6.
- Diboulo E, Sié A, Rocklöv J, Niamba L, Yé M et al. (2012) Weather and mortality: a 10 year retrospective analysis of the Nouna Health and Demographic Surveillance System, Burkina Faso. Global Health Action. 5:19078.
- Institut national de la statistique et de la démographie (INSD) (2015). Tableau de bord démographique. Ministère de l’Economie des Finances Burkina Faso. 1-61.
- Adebusoye LA, Cadmus EO, Owolabi MO, Ogunniyi A (2019) Frailty and mortality among older patients in a tertiary hospital in Nigeria. Ghana Med J, 53:210-6.
- Ministère de la Santé Burkina Faso, Organisation Mondiale de la Santé. Profil sanitaire complet du Burkina Faso. Ministère de la Santé Burkina Faso. 2017:1-50.
- Mcgregor G, Bessemoulin P, Ebi P, et Menne B. Vagues de chaleur et santé: guide pour l’élaboration de systèmes d’alerte. OMS, OMM.1-128.
