
Intestinal Necrosis due to an Incarcerated Internal Hernia Through a Peritoneal Defect in the Pouch of Douglas. Case Report and Literature Review
Mejía Solís Edwin Allen1, Juan Pablo1, Flores Sobreyra1, Monserrat Ashanti Vela Ramos1, Pierre Jean Aurelus2*
1Department of General Surgery, Regional Hospital of ISSSTE, Puebla, Mexico.
2Department of Gastro-transplantation, Pediatric Hospital of CMNSXXI (IMSS), México.
Received Date: December 28, 2018 ; Accepted Date: 04 January, 2019; Published Date: 14 January, 2019
Corresponding Author: Pierre Jean Aurelus, Hospital de Pediatría Centro Médico Nacional Siglo XXI (Instituto Mexicano Del seguro Social “IMSS”), México. Tel: +525556276900; Email: aurelusjean@yahoo.com.mx
Abstract
Background: Internal hernia through the pouch of Douglas is extremely rare. It is more frequent in women over sixteen years old. There are few reports of internal hernia through Douglas Pouch in the literature nevertheless in elderly, what is the main to present this work of intestinal necrosis in an elderly woman in the ISSSTE of Puebla Hospital.
Case Presentation: A 89-year-old woman was presented to the emergency department of ISSSTE Hospital. She had history of abdominal surgery, hysterectomy due to uterine myomatosis. She was admitted due to intermittent abdominal pain, abdominal distension and vegetative symptoms. Her physical examination revealed: dehydration, abdominal mild distension, hyperactive bowel sounds and peritoneal irritation data’s. Abdominal X-ray and Abdominopelvic tomography (CT) were performed.
Surgical Procedure: Exploratory laparotomy was performed; the abdomen was opened through a midline incision supra and infraumbilical. Underwent, resection of necrosis zone, previous the reduction of the small bowel; intestinal anastomosis laterolateral (jejunum and ileum) with 2 zero vicryl under Connell Mayo and Lembert points were performed. Reparation of pouch of Douglas was performed with vicryl suture 2 zero. Furthermore, peritoneal washed of abdominal cavity was performed and three drainages were inserted.
Outcomes: the patient had not improvement; at day 9 of the procedure she presented an acute hemodynamic deterioration without recuperation despite the management.
Conclusion: The internal hernia of the Pouch of Douglas is rarely and its mortality is high in elderly woman without an early diagnosis like it was in this case.
Keywords: Intestinal necrosis; Internal Hernia incarcerated; Pouch of Douglas
Introduction
Internal hernia through the pouch of Douglas is extremely rare, it is considered like the protrusion of an intestinal part into a large fossa in abdominal cavity. It has an incidence between 0.5 % to 4% and most of 50% of mortality [1, 2]. However, this infrequently internal hernia, it is more frequent in women over sixteen years old and it is diagnosed preoperatively due to nonspecific symptoms and signs with imaging findings. The internal hernias have been classified in: paraduodenal hernia that represented 53% of cases, perineal hernia (13%), Winslow foramen (8%), transmesenteric and transmesocolic hernia (7%), intersigmoidal hernia (6%) [1-3]. Frequently the internal hernia is occurred secondary to weakening of the pelvic floor musculature. On the other hand, there are few reports of internal hernia through Douglas Pouch nevertheless in elderly patient, what is the main to present this work of intestinal obstruction with necrosis in an elderly woman in the ISSSTE (Institute of Security and Social Services of State Workers) of Puebla Hospital due to an incarcerated internal hernia.
Case Presentation
A thin elderly woman of 89-year-old, with 40 kg of weight (BMI 18kg/m2) and 1.48cm of height was presented to the emergency department of ISSSTE Hospital. She had history of abdominal surgery, hysterectomy due to uterine myomatosis. She was admitted with history of 5 days of intermittent abdominal pain, abdominal distension and vegetative symptoms: nausea, persistent vomiting and tachycardia which started few hours ago. Her physical examination revealed: dehydration, abdominal mild distension, hyperactive bowel sounds and peritoneal irritation data’s. Abdominal X-ray showed a dilated small bowel loop, edema and air fluid levels suggestive of small bowel obstruction. Abdominopelvic tomography (CT) was performed and showed diffuse dilation in proximal to mild ileal loop with abrupt luminal narrowing at distal ileum level with evidence of bowel ischemia and thickening intestinal wall. However she had mechanical obstruction pattern with bowel perforation due to free air showed in both images studies. The diagnosis of intestinal obstruction was entertained and a nasogastric tube was inserted; furthermore, intravenous hydratation and antibiotics therapies were administered and immediately exploratory laparotomy was indicated (Figures: 1, 2).
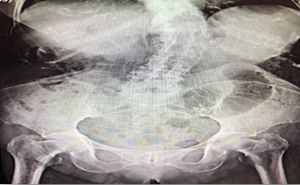
Figures 1: Preoperative X-ray. Small intestinal dilated.
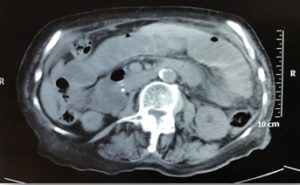
Figure 2: Abdominopelvic CT image.
Surgical Procedure
Under those characteristics of peritoneal irritation data’s, exploratory laparotomy was performed, the abdomen was opened through a midline incision supra and infraumbilical. The small bowel was reviewed from treitz angle to the ileocecal junction; at the pouch of Douglas in his flexure a perforation of three cm of diameter was localized with incarceration of approximately 120 cm of small bowel loop with a large necrosis zone approximately 80% of its intestine and an evidenced area of intestinal perforation were showed. Furthermore, proximal intestinal is dilated and distal collapsed small bowel. Underwent, resection of necrosis zone, previous the reduction of the small bowel; intestinal anastomosis laterolateral (jejunum and ileum) with 2(0) vicryl under Connell Mayo and Lembert points were performed. Reparation of pouch of Douglas was performed with vicryl suture 2(0). Furthermore, peritoneal washed of abdominal cavity was performed and three drainages were inserted. The procedure duration was 240 minutes (Figures 3, 4).
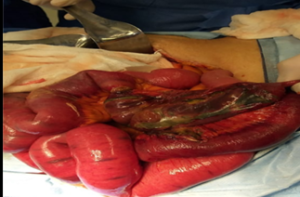
Figure 3: Large necrosis zone of small intestinal.

Figure 4: Large necrosis zone of small intestinal.
Outcome
The patient showed no improvement due to hemodynamic instability and sepsis with hypotension that were managed with antibiotics, noradrenalin, intravenous hydratation and intravenous nutrition. She had satisfactory recovery in the first three days of post operatory. However, on her 5rd hospital stay, the patient had showed greatest hemodynamic disturbance, and distension abdominal; for that, CT abdominal was performed without evidence of collection and perforation intestinal in this study. Therefore, she continued without improvement and at day 9 of the procedure she presented an acute systemic impairment without recuperation (Figures: 5, 6).
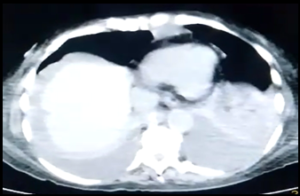
Figure 5: Postoperative TC
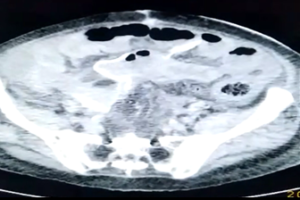
Figure 6: Control TC. Without free air fluid.
Discussion
The pouch of Douglas is anterior reflex of the peritoneum from the uterus to the rectum that is known like recto-uterine bag. Furthermore, history of multiples pregnancies or deliveries, previous operation and the old age may weaken the musculature in this anatomic space and induced internal hernia [2]. However, some studies, reported that the basis of the hernia was assumed to be Hysterectomy in woman, congenital and indeterminate causes [1-3]. In fact, this patient had previous surgical procedures, and she was an older woman and multiples pregnancies in her young life and she was admitted with a lately diagnosis. However, in this patient the bowel was herniated through a defect in the pouch of Douglas that may be associated to the previous hysterectomy.
Tomography data’s of an internal hernia in the pouch of Douglas showed static and dilated intestinal loops trough the pelvic region with thickening intestinal wall and pneumatosis; like it was showed in this older patient[3,4]. However, by the weakness of the muscle in this zone it is controversial to use or not a prosthetic material. It should be mentioned, in this patient, it was better performed a primary closure of the defect without used a prosthetic material [3-6]. In fact, the surgical treatment in internal hernia in the pouch of Douglas consists in the reduction of the bowel incarcerated and closure of the defect by non absorbable suture. However, in older patient the following may be not satisfactory due to various and high level of co-morbidities like they were in this patient [5, 6].
Generally, the main symptom of internal hernia is the distension abdominal due to small bowel loop occlusion and dilatation, it is indicated the CT abdominal previous an X-ray to perform the diagnosis; even though, the diagnosis would be intraoperative rather than preoperative and the management it is under an exploratory laparotomy as it was in this patient. Therefore, the following is depending of the co-morbidity of the patient and the length of the necrosis small bowel. In fact, this patient had a large loop of intestinal necrosis due to the incarcerated internal hernia that caused an inadequately following despite the early medical and surgical managements [2-4].
Conclusion
The internal hernia in the Pouch of Douglas is rarely in the general population with an incidence mayor in the woman elderly and it has a high mortality when it is present with intestinal necrosis, and a delayed diagnosis like it was in this case. Like mentioned in other literature, all diagnosed cases in this entity should be published.
Conflicts of Interest: There are no conflicts of interest to disclose.
Acknowledgements: To ISSSTE, Patient, Mejía Family.
Sites: ISSSTE (Institute of Security and Social Services of State Workers) Puebla/Mexico; Centro Médico Nacional Siglo XXI “Hospital de Pediatría Dr. Silvestre Frenk Freund.” Department of Gastro-transplantation/Instituto Mexicano del Seguro Social (IMSS)/México
References
- Muthukumar V, Venugopal S, Subramanian SK (2017) Report of a case and Review of Literature of Internal Hernia through Peritoneal Defect in Pouch of Douglas: A Rare Occurrence. Int. J: ApplBasic.Med.Res 7: 196-98.
- Stamatiou D., Skandalakis JE, Skandalakis LJ, Mirilas P (2010) Hernia perineal: anatomía quirúrgica, embriología y técnica de reparación. El cirujano estadounidense 76: 474- 479.
- Yutaka Inoue, Takashi Shibata y Takeshi Ishida (2002) CT of internal hernia through a peritoneal defect of the pouch of Douglas. American Journal of Roentgenology. 2002; 179(5).
- Alfredo Moreno Egea Fernando Carbonell Tatay, capítulo 57, Hernias abdominales internas.693
- Katsuhito Suwa, Tetsuya Yamagata (2013) Internal hernia through a peritoneal defect in the pouch of Douglas: Report of a case. Int J Surg Case Rep 4: 115-117.
- Choi Pyong Wha. Small Bowel Obstruction Caused by Internal Hernia through a Peritoneal Defect of the Pouch of Douglas: Report of a Case and Review of the Literature. Hindawi Case Rep Surg. 2017; 1-3
Citation: Allen MSE, Pablo J, Sobreyra F, Ramos MAS, Aurelus PJ (2019) Intestinal Necrosis due to an Incarcerated Internal Hernia Through a Peritoneal Defect in the Pouch of Douglas. Case Report and Literature Review. Journal of Surgery, Operative Techniques and Anaesthesia. Jr Surg and Ane: JSAA-107.